Of all common neurological disorders, traumatic brain injury (TBI) has the highest incidence and poses a substantial challenge to public health. TBI is increasingly being recognised as a chronic disease with long-term consequences, such as an increased risk of late-onset neurodegeneration. The first Lancet Neurology Commission on TBI, published in 2017, provided expert recommendations to reduce the global burden of TBI, calling for concerted action. The Commission provided the foundation for subsequent research, informed strategies of major funding organisation, and has been used to brief legislators and inform policy.
There has clearly been substantial progress in the past 5 years. However, many of these advances have yet to achieve routine clinical implementation, and major issues persist, particularly in the care of patients with TBI in low-income and middle-income countries. This update to the Commission presents advances and discusses persisting and new challenges in prevention, clinical care, and research into TBI.
The FDA has cleared Abbott’s laboratory blood test for concussion, making it the first commercially available test of its kind, according to a company press release.
The Alinity i traumatic brain injury test measures two serum biomarkers that are closely associated with brain injury and provides results in 18 minutes. Those with a negative test would be able to avoid a CT scan and may be able to reduce their time waiting at a hospital, the release stated. The test can be used for adult patients within 12 hours of suspected injury.
FDA clears Abbott’s lab-based blood test to evaluate for concussion. Image: Adobe Stock
Because misdiagnosis of or undiagnosed TBI can exacerbate its short- and long-term effects, “providing tools that can objectively aid in the evaluation of a TBI or concussion is essential to giving people the answers and treatment they need,” the company said.
“People sometimes minimize a hit to the head, thinking it’s no big deal,” Beth McQuiston, MD, medical director in Abbott’s diagnostics business, said in the release. “Others wonder if a visit to the doctor or emergency room for a possible concussion will provide them with meaningful answers or care. Now that this test will be widely available in labs across the country, medical centers will be able to offer an objective blood test that can aid in concussion assessment. That’s great news for both doctors and people who are trying to find out if they have suffered a traumatic brain injury.”
According to Abbott, the Alinity i TBI test has a 96.7% sensitivity and complements the company’s i-STAT TBI plasma test, a rapid blood test for concussion previously cleared by the FDA in 2021.
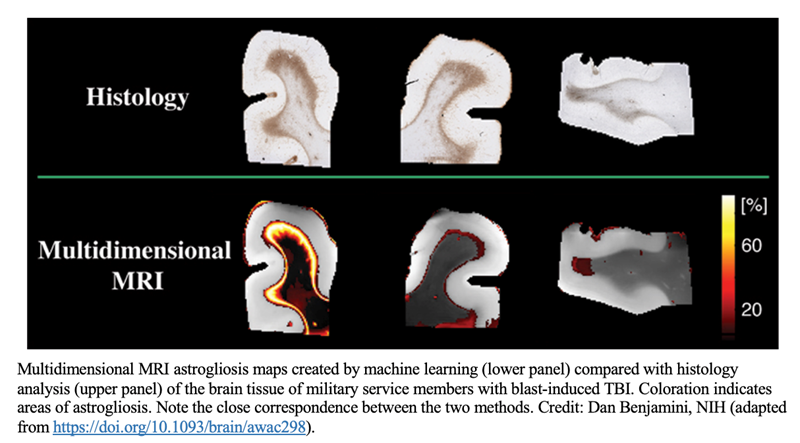
A National Institutes of Health (NIH)-developed multidimensional MRI method can detect astrogliosis, a neuroinflammatory response that occurs in traumatic brain injury (TBI) and other neurological conditions, according to a study published in Brain. Researchers had previously established that the multidimensional MRI strategy can identify diffuse axonal injury—a microscopic brain injury that, like astrogliosis, cannot be detected by conventional radiological methods.
The two studies, conducted with postmortem human brain tissue, illustrate the potential of using multidimensional MRI with living humans to identify biomarkers for diseases and disorders previously considered radiologically invisible.
The multidimensional MRI method was developed in the laboratory of Peter Basser, PhD, at NIH’s Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). The studies were conducted through a collaboration between NIH, the Center for Neuroscience and Regenerative Medicine (CNRM), and the Henry M. Jackson Foundation for the Advancement of Military Medicine. They were led by Dan Benjamini, PhD, a former NICHD postdoctoral fellow in Dr Basser’s lab and CNRM staff scientist who is now a tenure-track investigator at NIH’s National Institute on Aging.
Conventional MRI methods lack the sensitivity to detect microscopic brain injuries such as axonal injury and astrogliosis. Diffuse axonal injury is a type of TBI that involves tearing of the brain’s white matter fibers when the brain shifts and rotates inside the skull. Astrogliosis is an abnormal increase in the number and size of reactive astrocytes that can occur in TBI, neurodegenerative diseases and disorders such as epilepsy and multiple sclerosis, aging-related diseases such as Alzheimer’s disease, and other neurological conditions.
MRI methods that can detect such microscopic changes would have potential research and clinical applications, including facilitating diagnosis of TBI, a major global public health concern.
To identify MRI biomarkers for astrogliosis, the researchers compared samples of postmortem brain tissue from seven military service members who had sustained TBI from blast exposure, which results in astrogliosis, and from seven people who had not. The researchers found that astrogliosis induces microscopic changes in the brain tissue that result in a distinct multidimensional MRI pattern. They then developed an approach to compare areas with and without astrogliosis in the same brain, allowing them to specifically map areas of astrogliosis. Their MRI results correlated well with findings from histology images—the current gold standard for detecting astrogliosis in tissue samples.
Their previous work to identify MRI biomarkers of diffuse axonal injury in human brain tissue samples followed a similar approach. Interestingly, they found that astrogliosis and axonal injury have opposite effects on certain parameters of their MRI spectra, suggesting that multidimensional MRI could be used to detect both conditions in the same brain.
If successfully adapted for use in live humans, this multidimensional MRI strategy could be applied to personalized diagnosis and therapy of TBI and other neurological conditions. It also would serve as a useful tool for neuroimaging studies of brain injury, disease, repair, and aging.
Additionally, the method can be used to identify other quantitative MRI biomarkers of injury or tissue damage. “In the past, finding potential MRI biomarkers was a shing expedition,” says NICHD’s Dr Basser. “Now we’re at least fishing with sonar.”
The scientists are now working to adapt their multidimensional MRI method to detect astrogliosis and other neurological diseases and disorders in people. In the future, they aim to conduct a small clinical study to validate the method.
Summary: A preclinical drug that inhibits the kinase enzyme Cdk5 may have the potential to treat depression, brain injuries, and disorders associated with cognitive impairment.
Source: University of Alabama Birmingham
James Bibb, Ph.D., and colleagues have described a novel preclinical drug that could have the potential to combat depression, brain injury and diseases that impair cognition. The drug, which notably is brain-permeable, acts to inhibit the kinase enzyme Cdk5.
Cdk5 is a crucial regulator of signaling in brain neurons. Over three decades of study, it has been implicated in neuropsychiatric and neurodegenerative conditions, including Alzheimer’s disease and Parkinson’s disease. Knocking out the enzyme in mice makes them resilient to stress, enhances their cognition, protects neurons from stroke and head trauma, and lessens neurodegeneration.
While inhibitors of Cdk5 could offer potential therapeutic benefits and new ways to study basic brain function, previous first- and second-generation anti-Cdk5 compounds largely get blocked at the blood-brain barrier that restricts movement of solutes from the blood to the central nervous system’s extracellular fluid. To date, no Cdk5 inhibitor has been approved to treat any neuropsychiatric or degenerative diseases.
Bibb and colleagues now report details of their anti-Cdk5, brain-permeable compound, 25-106. They also show that systemic administration of 25-106 alters neurobehavior in mice, reducing anxiety-like behavior.
“As perhaps the first robust systemic inhibitor, 25-106 represents an exciting and expandable and translatable pharmacological tool to study the function of Cdk5 activity in wild-type animals,” said Bibb, a professor in the University of Alabama at Birmingham Department of Surgery.
“Achieving systemic applicability may be considered a step forward toward the testing of Cdk5 inhibitors to treat neuropsychiatric and neurodegenerative diseases. This provides a promising landscape for future studies to assess the effects of brain-permeable Cdk5 inhibitors to combat stress, anxiety, depression, addiction, cancer and neurodegeneration.”
The study, “Systemic administration of a brain permeable Cdk5 inhibitor alters neurobehavior,” is published in the journal Frontiers in Pharmacology.
In the paper, researchers describe synthesis of the aminopyrazole-based inhibitor, and they used molecular modeling to show that 25-106 appears to occupy the same hydrophobic binding pocket as the well-established Cdk5 inhibitor roscovitine.
Cdk5 is a crucial regulator of signaling in brain neurons.
They showed that 25-106 inhibited Cdk5 activity in a dose-dependent manner in brain striatal slices ex vivo, and that it also penetrated the brain after systemic administration in mice to inhibit Cdk5 in vivo.
They measured the pharmacokinetic and pharmacodynamic parameters of 25-106 in blood plasma and the brains of mice, and the off-target distribution of 25-106 in the liver and kidneys.
Mice given systemic 25-106 showed modulated neurobehavior in the open field maze test and the tail suspension test, anxiolytic changes that have previously been linked to Cdk5 knockout mice.
They found that 25-106 is a non-selective inhibitor of both Cdk5 and another cyclin-dependent kinase, Cdk2, but note that very low levels of Cdk2 are found in the brain. However, any off-target or toxic effects of systemic inhibition of Cdk2 by 25-106 remain unknown.
A team of researchers at the Neuroscience Institute at Georgia State University has discovered that hidden differences in the properties of neural circuits can account for whether animals are behaviorally susceptible to brain injury. These results could have implications for the treatment of brain trauma.
People vary in their responses to stroke and trauma, which impedes the ability of physicians to predict patient outcomes. Damage to the brain and nervous system can lead to severe disabilities, including epilepsy and cognitive impairment.
If doctors could predict outcomes with greater accuracy, patients might benefit from more tailored treatments. Unfortunately, the complexity of the human brain hinders efforts to explain why similar brain damage can affect each person differently.
The researchers used a unique research animal, a sea slug called Tritonia diomedea, to study this question. This animal was used because unlike humans, it has a small number of neurons and its behavior is simple. Despite this simplicity, the animals varied in how neurons were connected.
Under normal conditions, this variability did not matter to the animals’ behavior, but when a major pathway in the brain was severed, some of the animals showed little behavioral deficit, while others could not produce the behavior being studied. Remarkably, the researchers could artificially rewire the neural circuit using computer-generated connections and make animals susceptible or invulnerable to the injury.
“This study is important in light of the current Obama BRAIN initiative, which seeks to map all of the connections in the human brain,” said Georgia State professor, Paul Katz, who led the research project. “it shows that even in a simple brain, small differences that have no effect under normal conditions, have major implications when the nervous system is challenged by injury or trauma.”
Data sources Medline, Embase, Cochrane Central Register of Controlled Trials, BIOSIS (from their inception to April 2012), conference abstracts, bibliographies of eligible articles, and relevant narrative reviews.
Study selection Two reviewers independently reviewed citations and selected eligible studies, defined as cohort studies or randomised control trials including patients with moderate or severe traumatic brain injury and evaluating the prognostic value of S-100β protein. Outcomes evaluated were mortality, score on the Glasgow outcome scale, or brain death.
Data extraction Two independent reviewers extracted data using a standardised form and evaluated the methodological quality of included studies. Pooled results were presented with geometric means ratios and analysed with random effect models. Prespecified sensitivity analyses were performed to explain heterogeneity.
Results The search strategy yielded 9228 citations. Two randomised controlled trials and 39 cohort studies were considered eligible (1862 patients). Most studies (n=23) considered Glasgow outcome score ≤3 as an unfavourable outcome. All studies reported at least one measurement of S-100β within 24 hours after traumatic brain injury. There was a significant positive association between S-100β protein concentrations and mortality (12 studies: geometric mean ratio 2.55, 95% confidence interval 2.02 to 3.21, I2=56%) and score ≤3 (18 studies: 2.62, 2.01 to 3.42, I2=79%). Sensitivity analysis based on sampling time, sampling type, blinding of outcome assessors, and timing of outcome assessment yielded similar results. Thresholds for serum S-100β protein values with 100% specificity ranged from 1.38 to 10.50 µg/L for mortality (six studies) and from 2.16 to 14.00 µg/L for unfavourable neurological prognosis as defined by the Glasgow outcome score.
Conclusions After moderate or severe traumatic brain injury, serum S-100β protein concentrations are significantly associated with unfavourable prognosis in the short, mid, or long term. Optimal thresholds for discrimination remain unclear. Measuring the S-100β protein could be useful in evaluating the severity of traumatic brain injury and in the determination of long term prognosis in patients with moderate and severe injury.
What is already known on this topic
Many indicators have been independently associated with prognosis after traumatic brain injury, but they are of limited clinical use when considered separately and current prognostic models do not have sufficient discriminative capacity to inform clinical decision making
S-100β protein concentrations have been shown to increase in blood and cerebrospinal fluid after a wide range of diseases or conditions leading to brain damage
S-100β protein serum concentrations correlate significantly with unfavourable prognosis in patients with moderate or severe traumatic brain injury, as defined by mortality, Glasgow outcome score ≤3, or brain stem death, with or without concomitant traumatic injuries
The association between serum concentrations of S-100β protein and prognosis was observed at discharge from intensive care and at one, three, and six months.
Serum threshold values ranging from 1.38 µg/L to 10.50 µg/L and from 2.16 µg/L to 14.00 µg/L were associated with 100% specificity for mortality and a Glasgow outcome score ≤3, respectively.
Helmets successfully prevent most cranial fractures and skull traumas, but traumatic brain injury (TBI) and concussions continue to occur with frightening frequency despite the widespread use of helmets on the athletic field and battlefield. Protection against such injury is needed. The object of this study was to determine if slosh mitigation reduces neural degeneration, gliosis, and neuroinflammation.
Methods
Two groups of 10 adult male Sprague-Dawleyrats were subjected to impact-acceleration TBI. One group of animals was fitted with a collar inducing internal jugular vein (IJV) compression prior to injury, whereas the second group received no such collar prior to injury. All rats were killed 7 days postinjury, and the brains were fixed and embedded in paraffin. Tissue sections were processed and stained for markers of neural degeneration (Fluoro-Jade B), gliosis (glial fibrillary acidic protein), and neuroinflammation (ionized calcium binding adapter molecule 1).
Results
Compared with the controls, animals that had undergone IJV compression had a 48.7%–59.1% reduction in degenerative neurons, a 36.8%–45.7% decrease in reactive astrocytes, and a 44.1%–65.3% reduction in microglial activation.
Conclusions
The authors concluded that IJV compression, a form of slosh mitigation, markedly reduces markers of neurological injury in a common model of TBI. Based on findings in this and other studies, slosh mitigation may have potential for preventing TBI in the clinical population.