You probably don’t have to look further than your local drugstore or beauty product supplier to know CBD has taken a starring role in everything from sparkling water and gummies to tincture oils and lotions. Some may even say that cannabidiol (CBD) — which, like THC, is a component of the cannabis plant, but doesn’t contain its psychoactive effects — is the “it” ingredient of our age.
You’ve probably also heard that CBD can help lessen stress, anxiety, and pain. “When people are in pain, they have a stress response, which causes an increase in cortisol and an increase in blood sugar,” says Veronica J. Brady, PhD, CDCES, a registered nurse and an assistant professor at the Cizik School of Nursing at the University of Texas in Houston. Relieving pain can help alleviate the stress response and improve blood sugar levels, as well as aid sleep, she says.
If you’re managing type 2 diabetes, it’s natural to be curious about whether CBD might help you manage those symptoms, too, to help stabilize your blood sugar. In fact, the prevalence of cannabis use increased by 340 percent among people with diabetes from 2005 to 2018, according to one study, which surveyed people on their use of cannabis (CBD or THC, in any form) in the previous 30 days.
But will popping some CBD gummies for diabetes work Some healthcare professionals say CBD may have a role to play, but it’s important to understand that the only health condition CBD has proved effective for is epilepsy in kids. The jury is unfortunately still out, owing to the lack of comprehensive research on CBD for diabetes.
Still, in the aforementioned survey, 78 percent of people used cannabis that was not prescribed by a doctor. “Diabetes patients might still use cannabis for medical reasons, but not have a prescription,” says Omayma Alshaarawy, MBBS, PhD, an assistant professor in the department of family medicine at Michigan State University in East Lansing, who led the study. Recreational use is another factor. She points to a separate study that found that more than 50 percent of people with medical conditions such as diabetes or cancer use cannabis recreationally.
How People With Type 2 Diabetes Are Using CBD
In Nevada, where Dr. Brady used to work as a certified diabetes educator, her patients with type 2 diabetes used CBD for nerve pain. She says patients would use CBD in a tincture or in oils that they rubbed on painful areas, including their feet. Patients could buy CBD at medical marijuana dispensaries, which would offer dosing instructions. “They worried about the impact on their blood sugars,” says Brady.
Ultimately, though, Brady says that her patients reported that CBD reduced their nerve pain and improved their blood sugar. She adds that those people who used CBD oils for nerve pain also reported sleeping better.
Heather Jackson, the founder and board president of Realm of Caring in Colorado Springs, Colorado, a nonprofit that focuses on cannabis research and education, senses a community interest in CBD for diabetes. “In general, especially if they’re not well controlled, people are looking at cannabinoid therapy as an alternative, and usually as an adjunct option,” says Jackson. Callers have questions about CBD for neuropathy pain, joint pain, gastrointestinal issues, and occasionally blood glucose control, according to a spokesperson for Realm of Caring.
The organization receives thousands of inquiries about cannabis therapies a month. It keeps a registry of these callers, where they live, and their health conditions. Jackson says that people with type 2 diabetes are not a large percentage of the callers, but they currently have 540 people with diabetes in their database.
Jackson says that Realm of Caring does not offer medical advice, and it does not grow or sell cannabis. Instead, it offers education for clients and doctors about cannabis, based on its ever-growing registry of CBD users, their conditions, side effects, and administration regimen. “We are basically educating,” says Jackson. “We want you to talk to your doctor about the information you receive.”
Scientific Studies on CBD and Type 2 Diabetes and Barriers to Research
Despite interest among people with type 2 diabetes, large, rigorous studies showing how CBD may affect type 2 diabetes are lacking, says Y. Tony Yang, MPH, a doctor of science in health policy and management and a professor at George Washington University School of Nursing in Washington, DC. Specifically absent are randomized controlled trials, which are the gold standard of medical research.
At the very least, a case report from 2021 suggests that CBD is unlikely to cause harm or worsen diabetes control. (The American Diabetes Association also stresses that CBD should not be considered a replacement for traditional diabetes management.)
Other research suggests the use of CBD for diabetes is indeed worth further study. For example, a small study in the United Kingdom looked at 62 people with type 2 diabetes and found that CBD did not lower blood glucose. Participants were not on insulin, but some took other diabetes drugs. They were randomly assigned to five different treatment groups for 13 weeks: 100 milligrams (mg) of CBD twice daily; 5 mg of THCV (another chemical in cannabis) twice daily; 5 mg CBD and 5 mg THCV together twice daily; 100 mg CBD and 5 mg of THCV together twice daily; or placebo. In their paper, the authors reported that THCV (but not CBD) significantly improved blood glucose control.
Other CBD research is still evolving. Some research on CBD for diabetes has been done in rats, which leads to findings that don’t always apply to human health. Other research has looked more generally at the body’s endocannabinoid system, which sends signals about pain, stress, sleep, and other important functions. Still other studies have looked at marijuana and diabetes, but not CBD specifically.
That there are so few studies of CBD in people with type 2 diabetes has to do with a lack of focus on CBD as an individual component. Historically, cannabinoids (a group of chemicals in the cannabis plant) have been lumped together, including CBD, THC, and more than 100 others. The 1970 U.S. Controlled Substances Act classifies cannabis as a Schedule 1 drug with the highest restrictions, according to the Alcohol Policy Information System. Currently, 38 states allow cannabis for medical use, and 24 states and the District of Columbia have passed legislation allowing cannabis for recreational use, per CNN.
The 2018 Farm Bill removed industrial hemp from the controlled substances list, clearing the way for more production and research of CBD. Meanwhile, growers and manufacturers are better able to isolate CBD, mainly by cultivating industrial hemp that is high in CBD and very low in THC, says Jackson. So, perhaps in the coming years, more research on CBD and diabetes will emerge.
How the FDA Views and Regulates CBD for Disease Treatment
Yet, as evidenced by a previously cited study, people with type 2 diabetes aren’t waiting for further study to hop on the trend. Brady says her patients have been open about using CBD, particularly the younger patients. She says one of her older patients was initially uncomfortable about buying CBD in the same shop that sold marijuana but eventually gave in. Brady adds that many people associate CBD with smoking marijuana, despite their distinctly different effects on the body.
The U.S. Food and Drug Administration (FDA) approved the first CBD medication in 2018, for treating childhood epilepsy. Currently, there is no other FDA-approved CBD medication for diabetes or any other condition, according to the FDA. In December 2018, the FDA said it was unlawful under the Federal Food, Drug, and Cosmetic Act to sell food or dietary supplements containing CBD. But in January 2023 the FDA concluded that a new regulatory pathway for CBD is necessary and that it intends to work with Congress to develop one.
“The FDA, for the time being, has focused its limited enforcement resources on removing CBD products that make claims of curing or treating disease, leaving many CBD products for sale,” wrote Pieter Cohen, MD, and Joshua Sharfstein, MD, in The New England Journal of Medicine. Dr. Cohen is an assistant professor of medicine at Harvard Medical School in Boston, and Dr. Sharfstein is the vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health in Baltimore.
Precautions for People With Diabetes Looking to Try CBD
For the CBD products already on the market, Jackson says it’s often difficult to know what’s inside. One study found that only 30 percent of CBD products were accurately labeled, with under- and over-labeling of CBD content, and some products containing unlisted chemicals such as THC.
Vaping liquids were the most commonly mislabeled CBD products in the study. The Centers for Disease Control and Prevention (CDC) warns that consumers should not purchase any vape products from unregulated and illicit markets or attempt to modify vape products outside of how the manufacturer intended. The Associated Press has shown that some CBD vapes have synthetic marijuana.
Jackson points out that CBD may affect certain cholesterol and blood pressure drugs, and research has detailed these interactions. Other side effects of CBD include tiredness, diarrhea, and changes in weight or appetite, the researchers write.
“What you put in your body is really important,” says Jackson, adding that’s especially true for people with major health conditions like diabetes. Jackson speaks from personal experience as a mom finding CBD treatments for her son’s epilepsy. She says consumers should ask manufacturers whether CBD products are free of mold, pesticides, and other toxins.
“There is little known about cannabis health effects, especially among patients with chronic conditions. Research is growing, but still solid evidence evolves,” says Dr. Alshaarawy. For these reasons, she recommends that patients talk to their doctors so they can discuss the benefits and potential harms of cannabis and monitor their health accordingly.
How to Talk to Your Healthcare Provider About Using CBD for Type 2 Diabetes
Jackson and Brady advise people who are considering CBD for diabetes to ask their providers about the complementary therapy before adding it to their treatment plan. Brady says it’s difficult to find research about CBD and type 2 diabetes, even in her capacity as a diabetes educator. Still, in her experience, if people are looking for a natural way to manage pain, it’s worth a conversation with their healthcare provider. “It’s something that should be talked about, especially if they’re having significant amounts of pain, or really any pain at all associated with their diabetes,” says Brady.
“It’s a reasonable alternative,” says Brady. “As it gains in popularity, there needs to be some information out there about it.
The way type 2 diabetes affects the spine may explain why people experience lower back pain.
People with type 2 diabetes are at high risk for several diseases and health complications, including back pain.
Researchers from the University of California San Diego and the University of Utah report that type 2 diabetes negatively impacts the vertebral discs that form the spine, via an animal model.
This finding could explain why people with type 2 diabetes often experience chronic body pain, including back pain.
Now, researchers from the University of California San Diego and the University of Utah report that type 2 diabetes negatively impacts the vertebral discsTrusted Source that form the spine.
Via an animal model, scientists found that type 2 diabetes causes the collagen fibrilsTrusted Source within discs to become inflexible, comprising their ability to withstand pressure.
The new study was recently published in the journal PNAS Nexus.
Past studies show that type 2 diabetes can adversely affect the body’s spine and back.
For example, people with type 2 diabetes are at an increased risk of developing diffuse idiopathic skeletal hyperostosis (DISH)Trusted Source. DISH is a type of arthritis that hardens the tendons and ligaments around the spine, causing stiffness, decreased motion, and pain.
Prior studies have shown that people with diabetes have a 35% increased riskTrusted Source of experiencing low back pain and a 24% heightened risk of having neck pain compared to those who do not have the disease.
“We wanted to see if the effects of diabetes we were seeing in the bones were also present in the vertebral discs, which could explain disc degeneration and low back pain in these populations,” Dr. Claire Acevedo, assistant professor in the Department of Mechanical and Aerospace Engineering at the University of California San Diego, adjunct assistant professor of biomedical engineering and mechanical engineering at the University of Utah, and co-lead author of this study explained to Medical News Today when asked why they decided to focus on the vertebral column for their study.
For this study, researchers used a rat model of type 2 diabetes. Vertebral discs from rats with type 2 diabetes were compared to healthy rats to look for any collagen fibril deformation in the discs. The outer portion of vertebral discs is made from layers of collagen and proteins.
The researchers discovered in rats with type 2 diabetes, the compression ability of the disc collagen fibrils became compromised, causing the collagen to become stiff and brittle and making it difficult for the collagen to handle being compressed like it would when healthy.
“Type 2 diabetes and the associated hyperglycemia (cross-links) the collagen fibrils more than usual, like a fast aging process.” — Dr. Claire Acevedo
“This increase in cross-linking limits the usual compression mechanisms — energy dissipation mechanisms — in the discs via one, limitation of the collagen fibrils deformation making the collagen more stiff and brittle, (and) two, limitation of the lamellar rotation,” Dr. Acevedo explained.
“Future treatment can target the cross-link removal to restore the disc’s ability to deform normally,” she added.
“Small angle X-ray scattering is an X-ray diffraction technique that enables (us) to measure the collagen fibril periodicity (67 nm). When we perform a tensile test in front of the X-ray beam, the collagen periodicity increases,” Dr. Acevedo said.
“We can capture this change in collagen periodicity, which allows us to calculate the collagen deformation or strain and measure the whole-disc deformation or strain at the same time,” she continued. “Therefore, we can see how much disc strain is transferred to the collagen level at the nanoscale.”
“Assessing AGEs content in discs or bones is complicated and intrusive while assessing AGEs crosslink increase in (the) skin might be a good way to assess the same increase in discs and bones, even though the absolute content value will differ between tissues,” she said.
MNT also spoke about this study with Dr. Neel Anand, an orthopedic surgeon and co-director of spine trauma at Cedars-Sinai Spine Center in Los Angeles.
Dr. Anand said he was not surprised by this study’s findings.
“Type 2 diabetes affects collagen — it’s a collagen disease and discs (are) collagen,” he explained. “The ring of the disc on the outside is made of collagen fibers. So it’s not surprising that it will affect the disc in some form, shape, or fashion.”
“Type 2 diabetes affects collagen all over the body. The collagen will get affected just like it affects the blood vessels in the body. That’s what type 2 diabetes does — that’s why you get vascular problems, you get heart problems, you get kidney problems. You get a million problems with type 2 diabetes, including eye problems, so it affects a lot of things.” — Dr. Neel Anand
However, Dr. Anand did point out this research was conducted through a rat model.
“Humans are not rats,” he continued. “Is (this) true in humans? (It) probably is — there’s probably some element to it. Someone’s got to prove that’s true in humans at some point. Ultimately, it has to translate to humans.”
People with obesity and type 2 diabetes lost more weight using daily periods of fasting than by trying to restrict calories over a six-month period.
Blood sugar levels lowered in people in both groups, and no serious side effects were observed.
Time-restricted eating, also called intermittent fasting, may be an effective weight loss strategy. Katecat / Adobe Stock
Around 1 in 10 Americans live with type 2 diabetes, a disease in which levels of blood glucose, or blood sugar, are too high. Diabetes can lead to serious health issues such as heart disease, nerve damage, and eye problems.
Excess weight is a major risk factor for the development of type 2 diabetes, and weight loss is often recommended for those with excess weight and type 2 diabetes. Calorie restriction—reducing overall calorie intake—is a mainstay of most weight loss programs. But such regimens are very difficult to stick with over the long term.
Time-restricted eating, also called intermittent fasting, has emerged as an alternative weight loss paradigm. In this approach, the time of day during which food can be eaten is restricted, but the amount or types of food are not. Small studies have suggested that intermittent fasting is safe and promotes weight loss in people with type 2 diabetes. But these studies only tracked participants for a short period of time. They also didn’t compare the approach with traditional calorie restriction.
In a new clinical trial, an NIH-funded research team led by Dr. Krista Varady from the University of Illinois Chicago compared fasting and calorie restriction for weight loss and blood-sugar reduction. They recruited 75 people with obesity and type 2 diabetes. Of these, 70 were either Hispanic or non-Hispanic Black—two groups in the U.S. with an especially high prevalence of diabetes. The participants were randomly assigned to one of three diet groups for six months.
The fasting group could eat anything they wanted, but only between the hours of noon and 8 pm. The second group worked with a dietitian to reduce their calories by 25% of the amount needed to maintain their weight. A control group did not change their diet at all. All groups received education on healthy food choices and monitored their blood glucose closely during the study. The results were published on October 27, 2023, in JAMA Network Open.
After six months, participants in the fasting group lost an average of 3.6% percent of their body weight compared to those in the control group. In comparison, people in the calorie-restriction group did not lose a significant amount of weight compared to the control group.
Both groups had similarly healthy decreases in their average blood glucose levels. Both also had reductions in waist circumference. No serious side effects, including time outside of a safe blood glucose range, were seen in either treatment group. People in the fasting group reported that their diet was easier to adhere to than calorie restriction.
“Our study shows that time-restricted eating might be an effective alternative to traditional dieting for people who can’t do the traditional diet or are burned out on it,” Varady says. “For many people trying to lose weight, counting time is easier than counting calories.”
Some medications used to treat type 2 diabetes need adjustment for time-restricted eating. Therefore, people considering intermittent fasting should speak with a doctor before changing their eating pattern.
People with type 2 diabetes treated with metformin plus a sulfonylurea with high affinity for cardiac mitochondrial adenosine triphosphate–sensitive potassium (mitoKATP) channels, such as glyburide and glipizide, had a significant, adjusted 18% higher relative rate of major adverse cardiovascular events (MACE) compared with matched patients who received a low-affinity sulfonylurea, such as glimepiride, in an observational study of more than 50,000 matched pairs of patients in Taiwan.
The increased MACE risk primarily was associated with hospitalization for myocardial infarction, and the risk was greatest during the first 90 days of treatment and with a high dose of a sulfonylurea with high mitoKATP channel affinity, write Meng-Ting Wang, PhD, and associates in a report recently published in JAMA Network Open.
These findings suggest that “the high-affinity blockage of cardiac mitoKATP channels may act as an important determinant of sulfonylurea-related adverse cardiovascular events in patients with type 2 diabetes,” conclude the authors, who are affiliated with several institutions in Taipei, Taiwan.
The findings both confirm and refine a long-standing suspicion that at least some agents in the sulfonylurea class may increase risk for cardiovascular disease events, although evidence for this adverse effect is largely considered inconclusive.
In part because of safety concerns like this ― as well as other relative shortcomings of sulfonylureas, such as weight gain and relatively higher rates of hypoglycemia — the drug class has dropped from secondary to tertiary agents in the hierarchy of antidiabetic drugs in some sets of treatment recommendations. Despite this, sulfonlyurea use persists, especially in lower-income countries but also in the United States, owing to the affordability of agents in this class.
For example, glimepiride sells at many US pharmacies for as little as $20 for as much as a 6-month supply, less than 1% of the full retail cost of many agents now favored for treating patients with type 2 diabetes, such as the sodium-glucose cotransporter 2 (SGLT2) inhibitors and the glucagon-like peptide-1 (GLP-1) agonists.
De-emphasizing Sulfonylureas
“This study is part of an ongoing series of observations suggesting some of the challenges of sulfonylureas in the management of diabetes,” commented Robert A. Gabbay, MD, PhD, chief scientific and medical officer for the American Diabetes Association (ADA).
The findings “suggest there may even be differences between specific sulfonylurea analogs,” Gabbay said in an interview. He also highlighted that the ADA’s annual Standards of Care in Diabetes―2023 management recommendations, as well as in recent prior editions, “de-emphasize” use of sulfonylureas “in favor of others that show cardiovascular benefits,” such as metformin, the SGLT2 inhibitors, and the GLP-1 agonists.
“Currently, two opposing opinions are present in the literature. Some people consider that there is almost no more place for sulfonylureas when taking into account alternative new medications that showed advantages compared with older agents,” wrote André J. Scheen, MD, PhD, in an assessment of sulfonylureas published in 2021.
“Others make a plea for maintaining a right place of sulfonylureas in the therapeutic armamentarium of type 2 diabetes, especially in countries with limited resources,” noted Scheen, professor and head of the Division of Diabetes, Nutrition, and Metabolic Disorders at the Academic Hospital of Liège, Belgium.
Low-Affinity Sulfonylureas Predominate in Taiwan
The new JAMA Network Open study used data from more than 670,000 people in the Taiwan Diabetes Mellitus Health Database from 2006–2017, which included essentially all people in Taiwan who were newly diagnosed with diabetes during that period. This cohort included more than 280,000 adults who received sulfonylurea as second-line treatment after metformin; nearly 248,000 of these people qualified for the analysis, mostly because at least 1 year of data were available for them.
The study cohort included about 193,000 on a low-affinity sulfonylurea, glimepiride, or gliclazide (the latter is not approved for US marketing) and 54,411 on a high-affinity sulfonylurea, glyburide, or glipizide. These four agents constitute more than 99% of the sulfonylureas prescribed for use with metformin for these Taiwanese adults during the study period.
These numbers indicate that in Taiwan during the 12 years studied, more than three quarters of people with diabetes who received a sulfonylurea added on top of metformin were on a low-affinity sulfonylurea associated with a lower risk for MACE.
The main analysis focused on 53,714 matched pairs of people from this study set, with one member of the pair on a low-affinity agent matched with someone on a high-affinity agent. The analysis also adjusted for demographic and clinical characteristics to further reduce the possible influence of confounding not resolved by matching.
The primary endpoint of MACE included cardiovascular death, hospitalization for myocardial infarction, and hospitalization for ischemic stroke during an average follow-up of about 10 or 14 months, depending on treatment subgroup.
The analysis showed that treatment with a high-affinity sulfonylurea was significantly linked with an 18% higher rate of MACE compared with those treated with a low-affinity sulfonylurea. This was primarily driven by a significant 34% relative increase in the rate of myocardial infarction among those who received a high-affinity agent. All-cause death in the high-affinity subgroup was a significant 27% higher among those who were taking a high-affinity agent compared with those taking a low-affinity agent. Plus, the rate of severe hypoglycemia was a significant 82% greater with high-affinity sulfonylureas compared with low-affinity agents.
The same team of researchers had previously reported largely similar findings in 2022 in Diabetes Care based on fewer people with type 2 diabetes in Taiwan, using close to 34,000 matched pairs of patients.
Type 2 diabetes is a chronic and progressive cardiometabolic disorder that affects more than 10% of adults worldwide and is a major cause of morbidity, mortality, disability, and high costs. Over the past decade, the pattern of management of diabetes has shifted from a predominantly glucose centric approach, focused on lowering levels of haemoglobin A1c (HbA1c), to a directed complications centric approach, aimed at preventing short term and long term complications of diabetes, and a pathogenesis centric approach, which looks at the underlying metabolic dysfunction of excess adiposity that both causes and complicates the management of diabetes. In this review, we discuss the latest advances in patient centred care for type 2 diabetes, focusing on drug and non-drug approaches to reducing the risks of complications of diabetes in adults. We also discuss the effects of social determinants of health on the management of diabetes, particularly as they affect the treatment of hyperglycaemia in type 2 diabetes.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial.
Request Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Diabetes, a chronic and progressive cardiometabolic disorder, is a major cause of morbidity, disability, and mortality worldwide. Comprehensive person centred management of diabetes requires attention to glycaemic control and risk factors for cardiovascular disease (hyperlipidaemia, hypertension, and tobacco use), weight management, early detection and treatment of microvascular, macrovascular, and metabolic complications of diabetes and mental health concerns, mitigation of burden of treatment, addressing social determinants of health, and improving quality of life.1 The past decade has seen multiple developments in each aspect of the management of diabetes. This review focuses specifically on recent advances in the management of hyperglycaemia in diabetes, including drug and non-drug treatments. People with diabetes, caregivers, clinicians, health systems, payers, and policy makers need to appreciate the complexity and cost associated with optimal care of diabetes to meaningfully improve the health and well being of people living with diabetes.
Epidemiology
The current prevalence of diabetes among adults is 10.5% worldwide (536.6 million adults), with marked variation across regions and countries, and is estimated to reach 12.2% (783.2 million adults) by 2045.2 Diabetes is more prevalent in high income (11.1%) and middle income (10.8%) countries than in low income countries (5.5%). The prevalence of diabetes is rising everywhere, most rapidly in middle income countries where the prevalence is expected to reach 13.1% by 2045,2 probably because of changing diet and lifestyle factors, rising rates of obesity, inadequate resources for early diagnosis and prevention, and potentially greater genetic or epigenetic susceptibility arising from inadequate fetal and childhood nutrition. Data for low and middle income countries are likely to be underestimated because of barriers to screening and timely diagnosis.
More than 90% of people with diabetes have type 2 diabetes,3 characterised by insulin resistance and progressive beta cell failure, and commonly associated with other cardiometabolic disorders, including obesity, hypertension, cardiovascular disease, and hepatic steatosis. Diabetes contributed to 6.7 million deaths in 2021 alone,4 highlighting the urgency of preventing diabetes and optimising its management to improve health outcomes and quality of life for all people at risk of or with the disease.1
Sources and selection criteria
We searched PubMed for articles published in English. We prioritised randomised controlled trials, clinical guidelines, consensus statements, and systematic reviews. Search terms were: ((type 2 diabetes mellitus AND management (medical subject headings (MeSH) terms)) AND (type 2 diabetes mellitus (MeSH terms))) AND (care management, patient (MeSH terms)). Filters applied were: clinical trial, guideline, meta-analysis, practice guideline, randomised controlled trial, and systematic review, from 1 January 2013 to 1 January 2023. The reference lists of these articles were screened for relevant publications.
Goals and targets of management of type 2 diabetes
The primary objectives of the management of diabetes are to reduce the incidence and burden of complications and to improve quality of life (figure 1). Historically, these objectives were pursued through control of hyperglycaemia. In this glucose centric approach, clinical practice guidelines recommend targeting haemoglobin A1c (HbA1c) concentrations at <7% (53 mmol/mol) or <6.5% (47.5 mmol/mol) and, more recently, continuous glucose monitoring time in range >70% for most non-pregnant adults with type 2 diabetes, with lower or higher glycaemic thresholds individualised for each person.5–7 These recommendations for levels of HbA1c come from data from randomised controlled trials showing a reduction in microvascular complications with more intensive glycaemic control,8–12 although data for the association between time in range and risk of complications of chronic diabetes are limited but emerging.13 Implementation of glycaemic targets based on continuous glucose monitoring has also been limited by gaps in insurance coverage and accessibility, although continuous glucose monitoring is increasingly recommended for and used by people with type 2 diabetes.14 15
Randomised controlled trials of older antihyperglycaemic treatments, such as sulfonylureas and insulins, however, have not shown a consistent association between intensive glycaemic control and reduction in macrovascular complications or mortality.16 Nevertheless, longer term follow-up of intensively treated adults provides some evidence of a lower risk of macrovascular events and cardiovascular death.8 17 Conversely, intensive glycaemic control in individuals with frailty, advanced age, and multimorbidity was associated with an increased risk of severe hypoglycaemia and death.18–20 Therefore, future research is needed to examine the effect of intensive glycaemic control when achieved with newer glucose lowering drugs, which have a lower risk of hypoglycaemia and additional cardio-reno-metabolic benefits. Taken together, these data highlight the importance of individualised glycaemic management and the need to shift the emphasis away from the imperfect surrogate of levels of HbA1c towards reducing hard outcomes of the adverse health effects of diabetes, while lessening the burden of treatment.21 22
Shifting pattern of management of type 2 diabetes. HbA1c=haemoglobin A1c; ASCVD=atherosclerotic cardiovascular disease; CKD=chronic kidney disease; HF=heart failure; GIP=glucose dependent insulinotropic polypeptide; GLP1RA=glucagon-like peptide 1 receptor agonist; SGLT2i=sodium glucose cotransporter 2 inhibitor; SU=sulfonylurea; DPP4i=dipeptidyl peptidase 4 inhibitor. *Insulin is preferred for acute management of severe hyperglycaemia; †Thiazolidinediones improve insulin resistance
Over the past decade, multiple randomised controlled trials have shown a reduction in cardiovascular disease, kidney disease, heart failure, and mortality with the use of glucagon-like peptide 1 receptor agonists (GLP1RAs) and sodium glucose cotransporter 2 inhibitors (SGLT2is), independent of a reduction in levels of HbA1c.23 These findings signalled a new complications centric era of the management of diabetes, focused directly on preventing or reducing macrovascular, microvascular, and other emerging complications of diabetes, such as heart failure. Many,6 24 25 although not all,26 clinical practice guidelines recommend treatment with GLP1RAs or SGLT2is, or both, for patients with cardiovascular or kidney disease, or both, or with risk factors for atherosclerotic cardiovascular disease, independent of glycaemic control, although all continue to stress the concurrent importance of achieving HbA1c targets.
More recently, the pattern of management of diabetes has begun to shift further, with a renewed focus on looking at the causes of type 2 diabetes and its metabolic comorbidities and long term complications. This pathogenesis centric approach places the management of obesity at the centre of the prevention and treatment of the disease.27 Even a relatively small amount (5-7%) of weight loss reduced the risk of incident diabetes and improved glycaemic control in people with type 2 diabetes.28–31 Greater amounts of weight loss have been reported to have greater beneficial effects on glycaemic control (including remission of diabetes), metabolic dysfunction, and quality of life.29 30 32–37 Weight loss achieved with metabolic surgery reduced the risks of microvascular and macrovascular complications of diabetes and reduced mortality.38–41
By contrast, intensive lifestyle treatments in the Look AHEAD (Action for Health in Diabetes) randomised controlled trial of 5145 adults with type 2 diabetes and overweight/obesity did not reduce the risk of cardiovascular events compared to usual care.30 The likelihood of detecting differences between the intensive lifestyle and conventional treatment groups might have been reduced because the cardiovascular event rate in the Look AHEAD population was much lower than anticipated (0.7% per year v estimated 3.1% per year).42 A post hoc analysis suggested that those who lost at least 10% of their body weight in the first year had a significantly lower risk of the primary outcome, which was a composite of the first occurrence of death from cardiovascular causes, non-fatal acute myocardial infarction, stroke, and hospital admission for angina (adjusted hazard ratio 0.79, 95% confidence interval 0.64 to 0.98, P=0.034).35 How weight loss achieved with drug treatment, particularly agents such as semaglutide and tirzepatide, compares with metabolic surgery for glycaemic control, microvascular and macrovascular complications, and mortality, should be examined.
Lifestyle treatments: medical nutrition treatment, physical activity, and sleep
Successful management of type 2 diabetes must include consistent attention to behaviours that sustain a healthy lifestyle and are foundational for achieving glycaemic control, preventing complications, supporting quality of life, and preserving optimal health. Medical nutrition treatment for diabetes emphasises a balanced selection of nutrient dense foods while minimising or eliminating added sugar, refined grains, and highly processed foods.6 7 43 Recommendations for optimal carbohydrate intake and composition vary, with the strongest evidence supporting an overall reduction in intake of carbohydrates. This principle can be applied to multiple dietary patterns, including a Mediterranean diet high in monounsaturated and polyunsaturated fats, low carbohydrate, vegetarian, or a plant based diets, and the Dietary Approaches to Stop Hypertension diet, with a focus on non-starchy vegetables, fruits, and legumes, and some dairy in those who are lactose tolerant.6 43 Only the Mediterranean diet has been shown to reduce cardiovascular disease and mortality.44 Also, evidence indicates the beneficial effects of involvement of community health workers to support education in self-management of diabetes and overall care, especially in rural or underserved communities, or both.45 Because hypertension and cardiovascular disease are major causes of mortality in individuals with diabetes, more attention needs to be paid to overall sodium intake and limiting the content of saturated fat and trans fat in the diet.6
Stopping smoking and abstinence from tobacco products is also imperative for cardiovascular health in adults with diabetes, and robust evidence supports the benefit of stopping smoking despite the potential for weight gain.6 46 Although nicotine replacement products and electronic cigarettes might facilitate stopping smoking, nicotine itself can impair glucose tolerance and adversely affect the cardiovascular system through increased sympathetic activation.47
Baseline levels of physical activity should be assessed to set reasonable and realistic behaviour oriented goals. Increasing the duration of physical activity and reducing sedentary time have been reported to improve cardiorespiratory fitness and HbA1c levels.48 Recommendations can be made to increase leisure time physical activity (walking, taking the stairs, and household chores), decrease sedentary time, and introduce physical activity on most days.6 49 Physical activities include both aerobic and resistance training, as well as flexibility and balance training.50
The length and quality of sleep are increasingly recognised as essential components of the management of diabetes and individuals should be screened for sleep related disorders.6 43 Referral for diagnosis and treatment of obstructive sleep apnoea and other sleep disorders should be considered if indicated. Screening for psychosocial factors and social determinants of health that might affect an individual’s diabetes care and quality of life should also be performed, with engagement of or referral to relevant clinical team members for further evaluation and care, as appropriate.43
Lifestyle interventions in individuals with obesity or who are overweight are most successful when efforts are intensive and frequent follow-up is available, either in person or virtually.6 49 Weight loss can be achieved in various ways, and is most effective when strategies are combined: caloric restriction, increased caloric expenditure, elimination or substitution of drugs that promote weight gain, use of weight reducing drugs and, in select individuals, metabolic or bariatric surgery. One dietary strategy that has received considerable attention in recent years is time restricted eating,51 although data in adults with type 2 diabetes are limited to one randomised controlled trial52 53 and a larger trial is ongoing (n=344; Using Early Time Restricted Feeding and Timed Light Therapy to Improve Glycemic Control in Adults With Type 2 Diabetes, NCT04155619). Weight management is discussed in more detail below.
Drug treatment of type 2 diabetes
Initial management of type 2 diabetes has traditionally included metformin in most adults because of its glucose lowering effect, neutral effects on weight, minimal risk of hypoglycaemia, safety profile, low cost, and ease of administration. Now, in the light of evidence from trials of cardiovascular and kidney outcomes, decisions on treatment of diabetes with drugs should be made based on cardiac comorbidities (established atherosclerotic cardiovascular disease and heart failure), risk factors for atherosclerotic cardiovascular disease and kidney disease, engaging adults in shared decision making, and prioritising the use of drugs shown to reduce the risk of cardiovascular or kidney adverse outcomes, or both, in adults with specific comorbidities.7 24–26
Adults with atherosclerotic cardiovascular disease or indicators of high risk
In people with established atherosclerotic cardiovascular disease or risk factors for atherosclerotic cardiovascular disease, a GLP1RA or SGLT2i with known cardiovascular benefit should be started, regardless of levels of HbA1c or background glucose lowering treatments.24 Drugs that have been shown to cause significant reductions in major adverse cardiovascular events in cardiovascular outcomes trials compared with placebo include the GLP1RAs dulaglutide (hazard ratio 0.88, 95% confidence interval 0.79 to 0.99), liraglutide (0.87, 0.78 to 0.97), and subcutaneous semaglutide (0.74, 0.58 to 0.95), and the SGLT2is canagliflozin (0.86, 0.75 to 0.97) and empagliflozin (0.85, 0.75 to 0.97).54–58 None of the trials of cardiovascular outcomes involved head-to-head comparisons of GLP1RAs versus SGLT2is.59
Individual components of the composite major adverse cardiovascular events outcome as well as secondary outcomes in the cardiovascular outcomes trials vary between GLP1RAs and SGLT2is. A reduction in stroke was seen in meta-analyses of randomised controlled trials of GLP1RAs compared with placebo (hazard ratio 0.83, 95% confidence interval 0.76 to 0.92) but not with SGLT2is compared with placebo (0.95, 0.85 to 1.05).59 The mechanisms and benefits of GLP1RAs and SGLT2is seem to be complementary, and evidence is emerging to support combination treatment, which might provide more benefit than each used alone.60–62 Currently, guidelines from the American Diabetes Association/European Association for the Study of Diabetes recommend the addition of the alternative class when more glucose lowering is needed.24 25
Adults with heart failure
GLP1RAs have not shown benefit for heart failure outcomes in individual randomised controlled trials of cardiovascular outcomes,55 56 58 although meta-analyses of these studies suggested a potential benefit.59 63 64 SGLT2is, by contrast, have consistently shown significant benefit for heart failure outcomes.54 57 65 Also, dapagliflozin and empagliflozin were beneficial in people with reduced or preserved ejection fraction without type 2 diabetes, and have an indication for improving heart failure outcomes.66–69 Accordingly, in people with heart failure, an SGLT2i with known benefit should be started to reduce the risk of major adverse cardiovascular events and worsening heart failure.24 26
Adults with chronic kidney disease
GLP1RAs have shown benefit for secondary kidney related outcomes in large individual randomised controlled trials55 56 70 and meta-analyses59 63 64 of cardiovascular outcomes, but dedicated kidney outcome trials are ongoing.71 Several SGLT2is, including canagliflozin, dapagliflozin, and empagliflozin, have shown benefit in adults with chronic kidney disease with or without type 2 diabetes and in dedicated kidney outcome trials, and have an indication for improving chronic kidney disease outcomes.24 72 Therefore, SGLT2is with primary evidence are preferred for individuals with an estimated glomerular filtration rate <60 mL/min/1.73 m2 or albuminuria, or both, to reduce the progression of chronic kidney disease. If SGLT2is are not tolerated or cannot be used, GLP1RAs with demonstrated renal benefit are a reasonable alternative.24 26 73 Current prescribing information allows SGLT2is to be started in adults with an estimated glomerular filtration rate of ≥20 mL/min/1.73 m2 for kidney benefit, although the glucose lowering effects are substantially reduced at an estimated glomerular filtration rate <45 mL/min/1.73 m2.74 A small reduction in the estimated glomerular filtration rate can be seen after starting treatment with SGLT2is because of reversal or correction of the previous hyperfiltration state in adults with diabetes, but it does not predict further reductions in estimated glomerular filtration rate or require discontinuation of treatment.
Role of metformin
Although metformin was a commonly used background drug in most large trials of cardiovascular and kidney outcomes,75 several post hoc analyses have demonstrated benefit with GLP1RAs or SGLT2is regardless of background use of metformin.76–82 Current guidelines from the American Diabetes Association/European Association for the Study of Diabetes and the American Association of Clinical Endocrinology no longer recommend metformin as the preferred first line agent for all individuals with type 2 diabetes, and instead suggest consideration of cardiac and kidney comorbidities when selecting first line treatment.6 24 25 Cost is a major consideration in selecting the most appropriate treatment, however, probably contributing to differences in these recommendations from guidelines used in other countries. In the US, insurers have not caught up with the guidelines, and require that metformin is used before other agents. Guidance from the National Institute for Health and Care Excellence (NICE) still recommends metformin as the first line treatment for people with cardiac or kidney comorbidities, or both, with introduction of an SGLT2i in people who cannot tolerate metformin or need intensification of treatment.26 Despite robust outcome data, GLP1RAs are not recommended ny NICE until failure of triple oral drug treatment and only in people with a high body mass index or in whom insulin treatment cannot be used.26 Insurance formulary restrictions on prescribing GLP1RAs and SGLT2is, including the requirement of step treatment starting with metformin, still persist but should be reconsidered to better align with scientific evidence.
Other situations when a drug other than metformin can be considered as first line treatment include severe or symptomatic hyperglycaemia (HbA1c>10%, ketosis, or weight loss), creatinine clearance or estimated glomerular filtration rate <30 mL/min/1.73 m2, or when the person cannot tolerate metformin despite slow up titration of the dose or a trial of the extended release formulation, or both. Sulfonylureas and thiazolidinediones are now less commonly recommended because of their adverse effect profiles. Sulfonylureas can lead to weight gain and are associated with a high risk of hypoglycaemia, and thiazolidinediones can also cause weight gain, as well as fluid retention and osteoporosis. People treated with thiazolidinediones must be monitored for the development of heart failure; thiazolidinediones are not recommended for those with symptoms of heart failure and are contraindicated in class 3 or 4 heart failure. Because generic forms of sulfonylureas and thiazolidinediones are available, however, these drug classes are options when cost is a barrier to accessing other agents or the individual’s clinical situation requires these drugs. Pioglitazone, a thiazolidinedione, has beneficial effects in hepatic steatosis and stroke, and can be considered in these contexts.6 83
Effect on weight and weight related comorbidities
Clinicians should also consider the effect of the glucose lowering regimen on weight and weight related comorbidities, including overweight or obesity and non-alcoholic fatty liver disease or non-alcoholic steatohepatitis. Weight loss is greatest with the dual glucose dependent insulinotropic polypeptide (GIP)-GLP1RA, tirzepatide, and subcutaneous semaglutide, followed by dulaglutide and liraglutide.27 Moderate weight loss is seen with the other GLP1RAs and SGLT2is. Drugs with neutral effects on weight include the dipeptidyl peptidase 4 inhibitors (DPP4is) and metformin, whereas the sulfonylureas, thiazolidinediones, and insulin all increase the risk of weight gain (table 1).24 27 84 Recent single centre and population based cross sectional studies in the US estimated that >70% of people with type 2 diabetes have non-alcoholic fatty liver disease and more than half of those with type 2 diabetes and non-alcoholic fatty liver disease have steatohepatitis.85–88 Insulin resistance, impaired lipid and glucose metabolism, and altered insulin secretion play a part in non-alcoholic fatty liver disease and progression of type 2 diabetes, and might indicate why the two diseases are so closely linked.89 Although limited evidence exists so far, current guidelines recommend the use of a GLP1RA or pioglitazone for the treatment of diabetes in people with non-alcoholic steatohepatitis.90 91 Weight management, which is essential for the treatment of hepatic steatosis, is discussed below.
In addition to choosing a drug that targets cardiovascular, kidney, and metabolic outcomes, clinicians should also develop a treatment approach that has sufficient efficacy to achieve glycaemic targets.24 Although some guidelines (most notably, the Australian Diabetes Society) cite a lack of evidence to support substantial differences in glucose lowering between antihyperglycaemic drug classes when used as monotherapy,92 prior meta-analyses, including a meta-analysis of 453 trials assessing nine drug classes, and the recently completed Glycemia Reduction Approaches in Type 2 Diabetes: A Comparative Effectiveness (GRADE) pragmatic randomised clinical trial comparing insulin glargine U-100, the sulfonylurea glimepiride, the GLP1RA liraglutide, and the DPP4i sitagliptin in 5047 individuals with moderately uncontrolled type 2 diabetes found insulin and GLP1RA to be significantly more effective at lowering HbA1c than the other examined drugs.93 ,94 The American Diabetes Association Standards of Care there categorise drug classes as having very high, high, or intermediate glucose lowering efficacy (table 1).24 The greatest reductions in levels of HbA1c are seen with the dual GIP-GLP1RAs, GLP1RAs, and insulin. In the GLP1RA class, subcutaneous semaglutide and dulaglutide had the highest efficacy for glucose lowering. The recently approved dual GIP-GLP1RA, tirzepatide, seems to have the greatest efficacy for reducing levels of glucose. SGLT2is and DPP4is have less robust HbA1c lowering effects and are classified as intermediate to high (SGLT2is) and intermediate (DPP4is).24 25 93
GRADE, a large scale, comparative effectiveness study of four drugs in combination with metformin, found that insulin glargine and liraglutide achieved and maintained HbA1c targets more effectively than glimepiride and sitagliptin. The study did not, however, include newer agents, such as the SGLT2is, or once weekly GLP1RAs.95 The GRADE study also highlighted the challenges of maintaining glucose targets over time, with 71% of study participants progressing to HbA1c ≥7% within four years, regardless of the treatment option.94 A meta-analysis of 229 randomised controlled trials comprising 121 914 participants suggested that glucose lowering efficacy was highest with GLP1RA and weakest with DPP4i, with other agents in between.96 By contrast, a meta-analysis of 140 randomised trials and 26 observational studies showed that each new class of non-insulin drugs added to metformin monotherapy lowers levels of HbA1c by about 0.7-1%.95 A shift towards earlier use of combination treatment, in contrast with a stepwise approach, to reach glucose targets and provide better glycaemic durability has been reported.24 97 For people with marked hyperglycaemia (eg, HbA1c >10% or with symptoms), clinicians should start insulin, or a combination of insulin with GLP1RAs.98 When improved glycaemic control is achieved, many people with type 2 diabetes can be safely transitioned to non-insulin treatments with close monitoring to prevent hypoglycemia and hyperglycemia.
Safety considerations
Other considerations in the selection of treatment for diabetes are the risks of hypoglycaemia, other adverse effects and safety considerations, as well as cost and administration requirements that often result in barriers to adherence. Therefore, individuals with diabetes, care partners, and clinicians need to engage in shared decision making to identify treatment strategies that are aligned with the individual’s goals of care, treatment preferences, the clinical and psychosocial context, and risks and benefits associated with each treatment option. Tables 1 and 2 summarise this information. Some key and controversial safety considerations are discussed below.
Safety and mitigation considerations for each drug class for type 2 diabetes
Acute pancreatitis
Acute pancreatitis has been reported in individuals who received GLP1RAs, DPP4is, and the GIP-GLP1RA, tirzepatide. After early post-marketing reports, the US Food and Drug Administration warned of a potential link between acute pancreatitis and GLP1RAs and DPP4is.99 Multiple preclinical, observational, and randomised controlled studies were inconsistent, with some showing positive associations and others showing no association.100 Ultimately, the FDA concluded that a causal relation could not be established and insufficient evidence existed to modify treatment. Systematic reviews and meta-analyses of randomised controlled trials (eg, long term cardiovascular outcomes trials) concluded that treatment with GLP1RAs or DPP4is was not associated with an increased risk of pancreatitis or pancreatic cancer.101–103
Nonetheless, current prescribing information, FDA guidance, and treatment guidelines recommend cautious use of these drug classes in people with a history of pancreatitis, in part because these people were excluded from most trials.24 If these drug classes are used, individuals should be monitored for signs and symptoms of pancreatitis and, if pancreatitis develops, treatment should be discontinued and not restarted.24 99 We also suggest caution in starting these drugs in people with a previous history of pancreatitis, particularly when the cause of pancreatitis is unknown or persists. Monitoring of lipase levels in randomised controlled trials showed asymptomatic fluctuations in both groups (intervention and placebo). Hence no evidence exists to suggest ongoing monitoring during treatment.
Gallbladder or biliary disease
GLP1RAs, DPP4is, and GIP-GLP1RAs are also associated with an increased risk of gallbladder and biliary disease, including cholelithiasis and cholecystitis.104–107 Although the absolute risk of biliary or gllbladder disease with GLP1RA therapy seems to be small, with a recent meta-analysis of 76 randomised controlled trials involving 103 371 103 371 participants reporting an additional 27 incidences per 10 000 patients per year,104 this finding might under-represent the true risk, because many studies did not report biliary related events. The risk seems to be higher with higher doses of drugs, longer duration of use, and when used for weight loss rather than glycaemic control. We therefore advise caution with the use of GLP1RAs, DPP4is, and GIP-GLP1RAs in people at high risk of biliary complications.
Diabetic retinopathy
A significant increase in retinopathy complications (3% v 1.8%, P=0.02), including vitreous haemorrhage, blindness, or need for photocoagulation treatment or an intravitreal agent, was seen in people receiving semaglutide during the SUSTAIN-6 (Trial to Evaluate Cardiovascular and Other Long term Outcomes With Semaglutide in Subjects With Type 2 Diabetes) randomised controlled trial with 3297 participants with type 2 diabetes.56 Of those with retinopathy complications, 83.5% had a history of retinopathy at baseline. In a meta-analysis of four cardiovascular outcomes trials of dulaglutide, liraglutide, oral semaglutide, and subcutaneous semaglutide, use of GLP1RAs was associated with an increased risk of rapidly worsening retinopathy (odds ratio 1.23, 95% confidence interval 1.05 to 1.44).108 In another meta-analysis, GLP1RAs were not independently associated with an increased risk of retinopathy, but an association between retinopathy and the magnitude of the reduction in levels of HbA1c was found.109 Rapid glucose lowering has previously been associated with worsening diabetic retinopathy,110 and the GLP1RA cardiovascular outcomes trials were not powered to detect differences in retinopathy complications. Thus whether worsening retinopathy is caused by the drug itself, a change or rate of change in glucose levels, or a combination of both is unclear. We advise caution when GLP1RAs are used, particularly semaglutide, in people with diabetic retinopathy, and individuals should be monitored closely for progression of retinopathy.111
Whether other GLP1RAs similarly increase the risk of progressive diabetic retinopathy is not known. Consultation with an ophthalmologist should be considered before starting GLP1RAs in people with pre-existing retinopathy.111 A large randomised controlled trial (A Research Study to Look at How Semaglutide Compared to Placebo Affects Diabetic Eye Disease in People With Type 2 Diabetes (FOCUS), NCT03811561) evaluating the long term effects of subcutaneous semaglutide on eye disease in 1500 people with type 2 diabetes is ongoing and should provide more evidence.
Amputations
An increased risk of lower limb amputations was first reported in the cardiovascular outcomes trial for canagliflozin that included 10 142 participants with type 2 diabetes and high cardiovascular risk (6.3 v 3.4 participants per 1000 patient years; hazard ratio 1.97, 95% confidence interval 1.41 to 2.75)57 and led to a warning added to the prescribing information for canagliflozin in 2017.112 The FDA removed the warning in 2020 based on more clinical trial data that found that the risk was less than previously described.113 Subsequent real world cohort studies, randomised controlled studies, and meta-analyses have reported conflicting results, with some suggesting an increased risk with all SGLT2is and others finding no increased risk.114–121 Therefore, reasonable steps to take are to consider factors that increase the risk of amputations before starting an SGLT2i, closely monitor people for lower limb ulcers or infections, and discontinue the SGLT2i if these occur. Subgroup and exploratory analyses of the SGLT2i cardiovascular outcomes trials, however, suggest cardiovascular benefit in patients with peripheral arterial disease,122–124 so clinicians should use shared decision making when assessing the benefits and risks of SGLT2is in those at high risk.
Diabetic ketoacidosis
SGLT2is are associated with an increased risk of diabetic ketoacidosis, particularly in people with type 1 diabetes and in the perioperative population.125 126 Rates in adults with type 2 diabetes are low and range from 0.16 to 0.76 events per 1000 patient years.127 In type 2 diabetes, the risk is increased in people who are insulin deficient, in older people, with prolonged use of SGLT2is, or in those with a combination of these factors.128 Guidance on risk management of diabetic ketoacidosis is mainly from individuals with type 1 diabetes, with little guidance specific to type 2 diabetes, and recommendations are mostly extrapolated from the type 1 diabetes context.126 129 People with diabetes should be informed of the importance of adherence to insulin treatment, avoiding very low carbohydrate diets (such as ketotic diets), and excessive intake of alcohol. Education on management of sick days should also be given, and insulin doses should be monitored carefully; basal insulin should not be discontinued completely during illness or planned activity, particularly in those receiving intensive insulin treatment.
Clinicians and people with diabetes should be aware of predisposing factors and the clinical presentation of diabetic ketoacidosis, which often occurs with lower serum glucose levels (so-called euglycaemic diabetic ketoacidosis), sometimes at glucose concentrations of ≤200 mg/dL (11.1 mmol/L). The SGLT2i should be discontinued and treatment started promptly if diabetic ketoacidosis is suspected. SGLT2is should also be discontinued 3-4 days before scheduled surgery, during prolonged fasting or low carbohydrate intake, or during critical illness to lessen the risk of diabetic ketoacidosis.24 Some have suggested that absence of ketosis (<0.6 mmol/L blood ketones, negative urine ketones) should be confirmed in people with type 1 diabetes before the start of treatment if SGLT2is are being used off label in this population,126 but no evidence exists in support of this practice for people with type 2 diabetes.
Starting and titrating insulin treatment
Many people with type 2 diabetes will eventually require insulin because of the progressive nature of the disease. For most people, a GLP1RA should be considered as the first injectable agent before basal insulin, based on the strong evidence of similar efficacy, beneficial effect on weight, and less hypoglycaemia.130 131 If more treatment is needed after a GLP1RA, basal insulin should be started first and titrated to a maximum effective dose in a safe and timely way.7 98 Several steps are necessary to support optimisation of insulin treatment, including clear communication of expectations, adequacy of glucose monitoring (including continuous glucose monitoring for people with basal insulin or intensive insulin treatment, and remote telemonitoring), a feasible dose titration plan, clearly defined glycaemic targets, and education on proper administration of insulin and storage.131–134 Whether the individual can self-titrate the dose or if more support is needed should be assessed. People who can self-titrate can be instructed to continue uptitrating the dose until fasting glucose levels are consistently between 80 and 130 mg/dL (4.4 to 7.2 mmol/L; or an individualised glycaemic target), an anticipated maximum basal dose is reached (eg, 0.5 units/kg/day), or have unexplained hypoglycaemia. Providing these endpoints is key to reducing the risk of being treated with an inappropriately high dose of basal insulin in an attempt to compensate for inadequate post-prandial glycaemic control (ie, overbasalisation) while facilitating continued titration to an effective dose.135 If the individual cannot self-titrate, consider providing weekly follow-up healthcare remotely (ie, telehealth) for timely dose titrations.
If the basal insulin dose has been sufficiently titrated but levels of HbA1c remain above the person’s individualised target or concern for overbasalisation exists, targeting postprandial glucose excursions is warranted. Initially, consider adding a GLP1RA or GIP-GLPRA if not already being used. The next step is to add prandial insulin as a separate injection or by switching to a fixed ratio combination. Basal bolus insulin treatment requires more injections, more glucose testing, more education, and carries a higher risk of hypoglycaemia and weight gain.98 Metformin or complication centric drugs (GLP1RAs and SGLT2is), or both, should be continued. Sulfonylureas should be discontinued because of the risk of hypoglycaemia with concurrent insulin treatment.
Weight management in type 2 diabetes
Among adults with diabetes in the US, almost 28% are overweight (body mass index 25.0-29.9), 46% have obesity (body mass index 30.0-39.9), and 16% have severe obesity (body mass index ≥40.0).136 Increasingly recognised as a chronic disease, obesity (termed adiposity based chronic disease)137 138 is characterised by excessive, maldistributed, and dysfunctional adipose tissue, and is associated with increased risks of hyperglycaemia (ie, prediabetes and type 2 diabetes), cardiovascular disease, hyperlipidaemia, hypertension, chronic kidney disease, cancer, urinary incontinence, non-alcoholic fatty liver disease, osteoarthritis, infertility, obstructive sleep apnoea, and gastro-oesophageal reflux disease.137
Obesity is closely related to the pathogenesis and pathophysiology of type 2 diabetes and it also affects the management and outcomes of diabetes.137 139 Strong evidence indicates that weight loss, particularly if >10% of body weight, can prevent, improve, and even reverse type 2 diabetes.140 The Diabetes Prevention Programme showed that people with prediabetes who were randomised to receive an intensive lifestyle intervention had a 16% reduction in the risk of progressing from prediabetes to diabetes for every kilogram of weight loss.37 In the Look AHEAD study of people with type 2 diabetes and overweight or obesity, improvement in fasting glucose and HbA1c levels was found with weight loss as little as ≥2 kg, and improvements were directly proportional to the amount of weight lost.31 After initial weight loss from lifestyle interventions or pharmacotherapy, compensatory physiological responses often make efforts at further weight loss more difficult, less successful, or difficult to maintain, a biological phenomenon referred to as obesity protecting obesity.141 Hence clinicians should provide a supportive approach, recognising personal biases, and avoiding stigma and judgment to facilitate weight management efforts.141
Despite years of commercial availability, obesity drugs are rarely used, with fewer than 5-10% of people with diabetes and obesity receiving obesity drugs in the US.142 This finding could be driven by the relatively low efficacy of historically available drugs for weight loss, with most drugs causing <7% body weight loss.141 Recent developments with incretin treatments have closed this gap, however, with up to 20% weight loss reported with tirzepatide.107 Several studies in people with obesity, with or without type 2 diabetes, treated with semaglutide or tirzepatide have reported reductions in body weight of at least 5-10% in up to 80-90% of people, and reductions of 15-20% in up to 40-50% of people.106 107 143 144 Efforts to lose weight in people with type 2 diabetes and obesity should be supported through preferential use of glucose lowering drugs that are associated with weight loss, avoiding glucose lowering and non-diabetes drugs associated with weight gain, and aiming for weight loss of 12-15% as appropriate, to achieve maximum benefits.7 140
Equity and affordability of diabetes care
Affordability, accessibility, and feasibility of implementing the diabetes care plan are major considerations in shared decision making. In the US, the high and rising costs of insulin and non-insulin drugs145 have contributed to diabetes distress,146 cost related non-adherence147 148 with a detrimental effect on diabetes health outcomes149 and rationing of other vital expenses.150 Therefore, healthcare providers must discuss concerns about affordability with all people with diabetes, ensure that prescribed drugs are available and accessible, and leverage care team and community support systems to reduce the financial burden of the management of diabetes.151 152
To deal with the growing concerns about affordability of insulin in the US, out-of-pocket costs have been capped in 2023 by the Centers for Medicare and Medicaid Services (which oversee publicly funded insurance for seniors, low income individuals, and people with disabilities or end-stage kidney disease), several private insurance plans, and insulin manufacturers, and the effect of these changes on cost related non-adherence and rationing will need to be assessed. The cost of drugs is generally much lower outside of the US because of highly regulated policies on drug pricing and cost effectiveness in other high income countries,153 154 but 80% of people with diabetes live in low and middle income countries155 and half do not have access to recommended diabetes treatments.156 These findings call for multifaceted policy solutions to lower costs, increase supply, and improve accessibility of evidence based diabetes treatments and technologies in all settings and populations.157
Socioeconomic barriers to optimal management of diabetes are multifaceted and include not only the high costs of diabetes drugs, technology, and equipment, but also foundational social determinants of health, such as the home environment with access to healthy food choices and space for physical activity, environmental pollution and endocrine disrupting chemicals, stable housing with access to electricity and refrigeration, employment type and stability, and educational attainment.152 Geographical differences in the quality of care and prevalence of type 2 diabetes and its complications exist across levels of rurality,158 159 neighbourhood disadvantage,158 160 and geopolitical environment.161–163 Several interventions have been shown to be successful in improving the management of diabetes, including community health worker programmes, diabetes prevention and self-management programmes adapted specifically to the needs of underserved and disadvantaged populations, expansion of health insurance as part of the Affordable Care Act, food and housing support programmes, and others.152
We must also be cognisant of pervasive racial and ethnic inequalities in the quality of diabetes care and health outcomes. In the US, racial and ethnic minority populations are disproportionately affected by diabetes164 and its complications.152 165 166 Multiple studies have shown worse glycaemic control165 167 168 and higher rates of acute complications (hypoglycaemia,160 165 169–172 diabetic ketoacidosis, and hyperglycaemic hyperosmolar state),160 165 170 173 chronic complications (kidney disease,165 174–178 amputation,165 175 cardiovascular disease,165 175 and retinopathy),176 179 and mortality180 181 among black people with type 2 diabetes relative to other racial and ethnic groups. People with type 2 diabetes from racial and ethnic minority groups are also substantially less likely to be treated with GLP1RAs and SGLT2is than non-Hispanic white people.182 183 Similar inequalities in the prevalence, management, and health outcomes of diabetes have been described in Europe184 185 and around the world.186 187 These inequalities highlight the need for structural solutions and multisector collaborations that deal with the barriers to optimal diabetes management and health at all levels to ensure that all people, regardless of race, ethnic group, socioeconomic status, or place of residence, receive high quality care.
Conclusions
The paradigm of diabetes management has shifted over the past decade from a predominantly glucose-centric approach to approaches that prioritise prevention of diabetes complications and addressing the underlying causes of diabetes and metabolic dysfunction, such as obesity (figure 2). High quality, evidence based management of diabetes therefore requires reducing glucose levels to a safe, patient centred range; using glucose lowering drugs with a strong evidence base for reduction of diabetes complications and excess adiposity, not just lowering levels of HbA1c; minimising burden of treatment and improving quality of life; and implementing care delivery models that support high quality (effective, efficient, safe, equitable, timely, and person centred) care.188 Access and affordability remain major barriers, as is the sustainable implementation of effective lifestyle interventions.
Person centred goals of treatment of type 2 diabetes
Questions for further research
What are the short term and long term health outcomes associated with combined GLP1RA and SGLT2i treatment?
What is the optimal weight loss target (>10% or 15%) in the management of type 2 diabetes?
What is the comparative effectiveness and safety of drug treatments for obesity compared with metabolic surgery for long term metabolic, microvascular, and macrovascular complications?
How can effective lifestyle treatments for long term weight loss be implemented effectively, sustainably, and equitably?
What are effective and sustainable ways to engage people with diabetes, care partners, and communities in the prevention and management of diabetes to ensure equitable access to care?
How can structural barriers to optimal metabolic health be removed?
Researchers found lower levels of the protein RFX6 led to beta cells in the pancreas releasing less insulin. Lower RFX6 levels also led to structural changes in the DNA, specifically in sites that have known links to diabetes risk. Credit Donny Bliss/NIH
Nearly 35 million people in communities across the U.S. have type 2 diabetes (T2D), putting them at increased risk for a wide range of serious health complications, including vision loss, kidney failure, heart disease, stroke, and premature death.1 While we know a lot about the lifestyle and genetic factors that influence diabetes risk and steps that can help prevent or control it, there’s still a lot to learn about the precise early events in the body that drive this disease.
When you have T2D, the insulin-producing beta cells in your pancreas don’t release insulin in the way that they should. As a result, blood sugar doesn’t enter your cells, and its levels in the bloodstream go up. What’s less clear is exactly what happens to cause beta cells and the cell clusters where they’re found (called islets) to malfunction in the first place. However, I’m encouraged by some new NIH-supported research in Nature that used various large datasets to identify key signatures of islet dysfunction in people with T2D.2
Earlier studies have linked about 400 sites in the human genome to an increased risk for T2D. But most of them—more than 9 in 10—are primarily in noncoding stretches of DNA that control genes. As a result, it’s been hard to figure out exactly how those genetic variants that increase risk in the general population lead to the changes in individuals who go on to develop T2D.
In the new study, a team led by Marcela Brissova and Alvin C. Powers, Vanderbilt University Medical Center, Nashville, and Stephen C.J. Parker, University of Michigan, Ann Arbor, used sophisticated analytic approaches to study changes within pancreatic tissues and islets taken from donors who’d had early-stage T2D at the time of their death. They included tissues from donors without T2D to serve as a comparison.
To get a better understanding, they looked at the tissues in multiple ways, studying differences in their basic physiology, gene activity, and cellular-level structures. By integrating data on these observed differences with other types of data from prior studies, they showed that impaired function of beta cells is a hallmark of early T2D, reinforcing prior evidence. Other pancreatic islet cell types appeared mostly unchanged.
Their studies also showed that alterations in a particular gene network are key in early-stage T2D. The network, controlled by a protein called RFX6, cause pancreatic beta cells to malfunction. The researchers performed additional studies that showed lowering RFX6 levels led beta cells to secrete less insulin. Lower RFX6 levels also led to structural changes in the DNA, specifically in sites that have known links to diabetes risk. They expanded this finding by doing a population-scale genetic analysis. Using genetic information for more than 500,000 volunteers available in the UK biobank, they showed a causal link between lower levels of RFX6 and T2D.
Further study is needed to understand what’s behind the initial changes in RFX6. The researchers also want to explore further whether RFX6 might be a promising target for new treatments to prevent or reverse early-stage molecular and functional defects in the beta cell that underlie T2D. The researchers note that they have made all the data publicly available through user-friendly and interactive web portals, in hopes it will lead to more answers for the millions already affected by T2D and so many others who may be at risk.
Diabetes is a chronic condition that impacts how the body processes glucose (sugar).
Diet is a critical component of diabetes management, particularly among people with type 2 diabetes.
A recent study found that following a high quality, low carb diet may reduce mortality risk among people with type 2 diabetes.
Diabetes management involves looking at multiple aspects of health, including diet and exercise levels. People with diabetes can work with their doctors and other specialists to create a treatment plan that fits their needs.
Researchers are still working to understand what diet choices align with the best outcomes for people with diabetes. One area of interest is the intake of carbohydrates in the diet.
A recent study published in Diabetes Care found that following a low-carbohydrate diet may benefit people with type 2 diabetes.
Researchers found that following a low carbohydrate diet with high-quality macronutrients was associated with a lower mortality risk among people with type 2 diabetes.
DiabetesTrusted Source is a chronic condition that involves irregularities with the hormone insulin. In someone without diabetes, the body releases insulin so that the glucose from food can enter the body’s cells. From here, the cells can use the glucose for energy.
In someone with diabetes, the body’s response to or the amount of insulin changes. Glucose remains in the bloodstream at higher levels than in people without diabetes.
Diabetes can lead to long-term complications, so people with diabetes need to take proper management steps. A key component of diabetes management is dietTrusted Source.
Carbohydrates break down to glucose, meaning that people with diabetes need to be aware of the carbohydrates consumed and how they can impact blood glucose levels.
Registered dietitian and certified diabetes care and education specialist Nicole Anziani, at Cecelia Health in New York, not involved in the recent study, explained to Medical News Today:
“Carbohydrates impact blood sugar levels. Maintaining blood sugar levels by promoting a greater percentage of time in range, without large spikes, helps those living with diabetes stay healthier longer by preventing or delaying diabetes-related complications such as kidney disease, blindness, nerve damage, and blood vessel disease that can lead to heart attacks, strokes, and amputations.”
She added that “consuming healthy carbohydrates like whole grains, fruits, and vegetables is an important part of a healthy eating plan because they can provide both energy and nutrients, such as vitamins and minerals, and fiber.”
Researchers looked at diet in relation to all-cause mortality and mortality from cardiovascular disease and cancer. Diet was assessed for several factors, including carbohydrate intake amounts and the quality of macronutrients.
The researchers created a scoring system to look at different low-carbohydrate diets, including low-carb diets focusing on vegetables or animals and low-carbohydrate diets that were healthy or unhealthy.
The study found that adhering to a low-carbohydrate diet was associated with lower all-cause mortality. However, the benefits of adhering to a healthy, plant-based, low-carbohydrate diet were the most pronounced. This diet option was associated with lower all-cause, cardiovascular, and cancer mortality.
Study author Dr. Yang Hu explained the key study findings to MNT:
“Our study shows that among people with established type 2 diabetes, a low-carbohydrate diet may have differential health effects on mortality depending on its composition. Our analysis suggested that only low-carbohydrate diets that emphasize plant-sourced fat, plant-based protein, and high-quality carbohydrates, such as those from whole grains, fruits, and vegetables, were associated with significantly lower overall, cardiovascular, and cancer mortality.”
“Clinicians may find our results useful when providing dietary recommendations to diabetes patients,” he noted.
The researchers found that the benefits of following this diet may be most pronounced for those who follow certain lifestyle practices, including not smoking, engaging in moderate to vigorous exercise, and moderate alcohol consumption.
Anziani also commented that: “The study’s conclusion that following a healthier [low-carb diet] pattern has significant benefits in regard to mortality levels for patients with type 2 diabetes is compelling and can help providers design dietary protocols for their patients that benefits them both short- and long-term.”
This study did have several limitations. Firstly, the study does not show a causal relationship between the factors the researchers studied.
Secondly, the researchers acknowledge that people who adhered to a low-carb diet may have been more likely to incorporate other healthy practices like properly taking medications.
Thirdly, the average people who consumed a low-carb diet in the study still got between 30-40% of their energy intake from carbohydrates.
Thus, the researchers caution that the results may not apply to very low carbohydrate diets. Data did rely on participant reporting, which does introduce the possibility for errors in data collection.
Finally, researchers were limited by their sample, which was health professionals of European ancestry. Further studies could include more participant diversity to make findings more generalizable.
“Although our study examined the health effects of low-carb diets in people with diabetes, whether healthy low-carb diets could help prevent the development of major cardiometabolic disease including type 2 diabetes and coronary heart disease in the general population is still not clear,” Dr. Hu noted.
“It is also of great interest for future studies to assess the associations between long-term adherence to low-carb diets and weight change, because the low-carb diet is often promoted as an effective diet pattern for weight loss,” he added.
Ultimately, diabetes management involves careful work with professionals to ensure the best possible health outcomes.
Registered dietitian and nutrition consultant at Lasta, Barbara Kovalenko, not involved in the study, offered the following words of caution to MNT:
“It’s important to note that more research is needed to confirm this study’s findings and to investigate the long-term effects of low-carbohydrate diets on health outcomes in people with type 2 diabetes. Additionally, when making dietary changes, it is critical to consult with a healthcare professional or registered dietitian to ensure that nutritional needs are met and medications are managed appropriately.”
Incretin hormones contribute a major portion to the insulin secretory responses after meals in healthy people. The incretin effect describes the phenomenon that oral glucose elicits approximately threefold greater insulin responses than the elevation in glucose (achieved with glucose administered intravenously) alone.
The incretin effect is the result of nutrient-stimulated secretion of the incretin hormones glucose-dependent insulinotropic hormone (GIP) and glucagon-like peptide-1 and their insulinotropic effect (ie, the augmentation of insulin secretion at elevated plasma glucose concentrations). In patients with type 2 diabetes, this incretin effect is severely impaired or even absent.
It is the purpose of this commentary to highlight current knowledge in incretin research and to answer the question of whether and to which degree abnormalities in incretin hormone secretion and action accompany the development of type 2 diabetes or even contribute to this process.
Michael A.
Nauck
Irfan Vardarli
Juris J.
Meier
History of incretin
The reduced incretin effect in patients with type 2 diabetes was first noticed in 1967 and was clearly established in 1986.
Three types of questions arose from this finding. What is the mechanism behind the reduced incretin effect? Is the secretion or insulinotropic action of GIP and GLP-1 at fault? Are defects in the enteroinsular axis (the signaling system between the gut, from where incretin hormones are secreted, and the endocrine pancreas, the main target tissue that incretin hormones act on) important for the development and/or progression of type 2 diabetes? Can the pathophysiological characterization of the incretin system in type 2 diabetes provide clues for the development of new approaches for the treatment of this metabolic disease?
A severe impairment in the insulinotropic activity of GIP in type 2 diabetes explains the reduced incretin effect. A large cross-sectional study by Toft-Nielsen and colleagues comparing GLP-1 responses after meal stimulation suggested a reduced release of GLP-1 in patients with type 2 diabetes and, to a lesser extent, impaired glucose tolerance (“prediabetes”). This widely quoted study was sometimes interpreted to indicate a progressive loss in the capacity of GLP-1 secretion in the natural history of type 2 diabetes, starting from normal secretion as long as glucose tolerance was normal with slight impairments when IGT develops, with a further deterioration after the diagnosis of type 2 diabetes and little residual capacity for GLP-1 secretion when the condition has progressed.
The logical consequence was to replace a missing hormone by advocating incretin-based antidiabetic agents (GLP-1 receptor agonists or dipeptidyl peptidase-4 inhibitors). However, not all studies that have compared the secretion of GLP-1 in patients with type 2 diabetes and in matched healthy people come to the same conclusions. A recent meta-analysis suggested no uniform reduction in L-cell secretion between healthy and type 2 diabetic patients, but a large interindividual variation, in part determined by age, obesity and plasma levels of glucagon and free fatty acids. In nondiabetics, the amount of GIP and GLP-1 secreted is significantly correlated to the incretin effect in quantitative terms. Thus, a low secretion of GLP-1 may determine a reduced incretin effect on an individual level, but does not explain the reduced incretin effect in patients with type 2 diabetes by and large.
If secretion is not the culprit, is there any peculiarity regarding the action of incretin hormones in type 2 diabetes? As originally described using GIP of the porcine amino acid sequence, and later confirmed using synthetic human GIP, the endocrine pancreas shows very little secretory response, even if exposed to supraphysiological concentrations of GIP. This inability to respond to GIP appears to be acquired, since populations at high risk for developing type 2 diabetes do not display a similar defect. Basically, the response to GIP seems to be normal in any form of prediabetes (first-degree relatives, patients recovering from gestational diabetes, etc.), but after diagnosis (ie, with a fasting glucose ≥126 mg/dL), the incretin effect is reduced or lost, as is the ability to respond to exogenous GIP.
Most likely, the inability to elicit insulin secretory responses with GIP, even at hyperglycemia, is explained by a generalized impairment in beta-cell secretory capacity, as is typical for type 2 diabetes, no matter which stimulus is looked at (hyperglycemia, amino acids, sulfonylureas, etc).
Source: Michael A. Nauck, MD, PhD
Furthermore, rodent studies have suggested a down-regulation of the GIP receptor by chronic hyperglycemia. The fact that this defect becomes apparent when glucose concentrations rise above the normal level has raised the question of whether this phenomenon is reversible by glucose normalization. A recent study by Højberg and colleagues suggested that this may be the case. However, although the insulin secretory responses to GIP and GLP-1 were significantly improved, normalization was not achieved after improved glucose control.
Abnormalities in the incretin system accompany the development of type 2 diabetes and may contribute to the velocity of progression. Figure 1 depicts the natural history of developing type 2 diabetes and also the progression of the disease after the diagnosis has been made. Changes in insulin secretory capacity, based on homeostasis model assessment (HOMA) estimation of beta-cell function, and insulin sensitivity preceding the diagnosis were taken from a recent analysis by Tabak and colleagues. The development after the diagnosis of diabetes was based on analyses from the UKPDS and ADOPT study.
Regarding the secretion of GIP and GLP-1, we refer to our recent review indicating no general abnormalities in K-cell (GIP) and L-cell (GLP-1) secretion associated with a diagnosis of type 2 diabetes. The fact that in none of the studies examining prediabetic populations, insulinotropic GIP effectiveness was impaired, but after the diagnosis, uniformly, a severe inability to respond to GIP with secreting insulin was documented, is the basis for assuming a substantial drop in beta-cell responsiveness to GIP around the time of diagnosis, with no further changes afterward (Figure 1). In a recent review, we have explained reasons to assume that this inability to secrete insulin in response to GIP stimulation goes along with a general impairment of beta-cell function, which is demonstrable with most other secretagogues as well.
Whether this inability of the endocrine pancreas to respond to GIP contributes to the natural history of type 2 diabetes can only be evaluated by quantitative considerations. If a mechanism to stimulate insulin secretion after meals that normally contributes two-thirds of the overall secretory responses is at fault, this almost certainly has the effect to accelerate the progression of type 2 diabetes because without the additional incretin stimulus, overall insulin secretion should be further impaired.
In the case of GLP-1, the insulinotropic activity is somewhat reduced after the diagnosis of type 2 diabetes, and even worse under the condition of uncontrolled hyperglycemia compared with healthy controls. High pharmacological doses of GLP-1, nevertheless, have the potential to raise insulin concentrations and to suppress glucagon secretion, with the overall result of normalizing glucose concentrations in the fasting state and after meals over a wide range of patients with type 2 diabetes, ranging from those treatable with lifestyle modification (“diet and exercise”) to those requiring insulin treatments.
Thus, the “resistance” to GIP of the type 2 diabetic beta-cell can be overcome by a compensatory exposure to high concentrations of the incretin hormone, GLP-1. GLP-1 itself appears to be less important than GIP for postprandial glucose control in healthy people and does not seem to be involved in the pathogenesis of type 2 diabetes. However, because of its preserved efficacy in type 2 diabetes, GLP-1 is an effective agent to treat hyperglycemia in type 2 diabetic patients, with the added benefits of inducing weight loss and avoiding hypoglycemia.




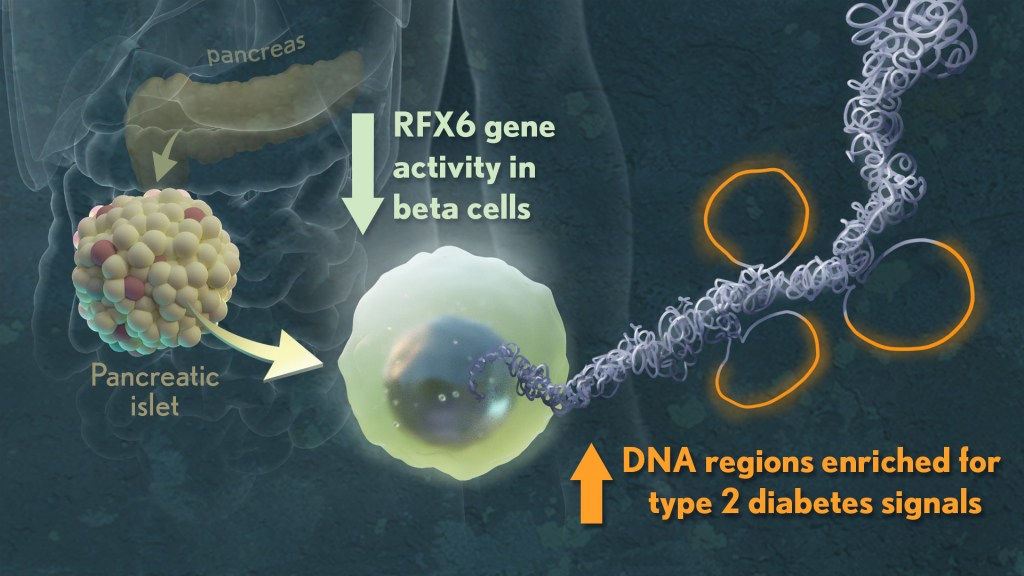






{kind=link}
{kind=link}
{kind=link}
{kind=link}