The antiviral drug Oseltamivir is very effective in treating uncomplicated cases associated with influenza A and influenza B viruses.[1] The drug can be used for the treatment of both adults and paediatric patients along with newborn babies and neonates less than 2 weeks old. Oseltamivir has been recommended as the drug of choice for the prophylactic treatment of influenza within 48 hours of the onset of symptoms in an infected person with significant comorbidities. However, Oseltamivir prophylaxis is recommended only for patients older than 1 year of age.
The World Health Organisation (WHO) and the Centers for Disease Control and Prevention (CDC) strongly recommend the use of Oseltamivir for the treatment and prophylaxis of disease resulting from avian influenza virus strains, including avian influenza A (H5N1).
Oseltamivir can be used for empirical treatment without confirmation of the disease and within 48 hours of the initiation of symptoms. This has been shown to reduce the duration of influenza in healthy people and hospitalised patients within 4-5 days of onset of symptoms. Oseltamivir is usually well-tolerated; however, the drug can produce certain adverse side effects like vomiting, nausea, abdominal pain, diarrhoea, insomnia, and vertigo in some cases.
Current smoking, use of sedative hypnotics and dyspnea increased the risk for death by suicide or drug overdose among adults with a smoking history with or without COPD, according to study results published in CHEST.
Further, risk for suicide in this patient population was not linked to airflow limitation, measured as FEV1 percent predicted, or other measures of COPD severity, according to researchers.
Data were derived from Adviento BA, et al. CHEST. 2022;doi:10.1016/j.chest.2022.09.022.
Karin F. Hoth
“An important aspect of our findings was that the objective measures of COPD severity (eg, airflow limitation from spirometry) that we examined were not associated with suicide/overdose, although symptom severity, specifically dyspnea, was,” Karin F. Hoth, PhD, associate professor of psychiatry at the University of Iowa, told Healio. “This finding suggests that the subjective experience of COPD is important in assessing suicide risk among individuals with smoking exposure. Further research is required to examine how COPD and current smoking interact on suicide risk and whether there is evidence of synergy between these two converging risk factors.”
In a prospective cohort study, Hoth and colleagues analyzed 9,930 adults (mean age, 59.6 ± 9 years; 53.4% men; 67.3% non-Hispanic white; 52.6% current smokers; mean BMI, 28.8 ± 6.3 kg/m2) with a 10-pack-year smoking history from the COPDGene Study to determine the factors that can predict suicide or drug overdose mortality in this patient population.
To evaluate time to suicide/overdose, researchers used Cox regression models that accounted for several time-varying independent variables in the past year: age, sex, race, BMI, pack-years, current smoking status, airflow limitation, dyspnea (modified Medical Research Council Dyspnea Scale score 2), 6-minute walk distance, supplemental oxygen use and severe exacerbations.
Results
Of the cohort, 12.4% of adults had preserved ratio impaired spirometry, 26.8% had mild to moderate COPD (Global Initiative for Chronic Obstructive Lung Disease [GOLD] 1-2), 17.6% had severe to very severe COPD (GOLD 3-4) and 42.5% had normal spirometry.
Additionally, 18.9% of adults used antidepressants, 10.1% used sedative/hypnotics, 3.5% used antipsychotics, 2% used mood stabilizers and 0.5% used stimulants. Fourteen percent of those with GOLD stage 3-4 COPD used sedative/hypnotics, which was the largest recorded use across groups.
Of the total cohort, seven adults died by suicide and 56 died by overdose for a total of 63 deaths during a median follow-up of 7.8 years.
Univariable models adjusted for age and sex demonstrated that race, BMI, current smoking status, use of sedative/hypnotics and dyspnea all significantly were linked to death of suicide or overdose.
In a multivariable model adjusted for univariable significant factors, age and sex, researchers observed several risk factors related to suicide/overdose mortality including a 6.44-fold (95% CI, 2.64-15.67) increased risk with current smoking, a 2.33-fold (95% CI, 1.24-4.38) increased risk with use of sedative/hypnotics and a 2.23-fold (95% CI, 1.34-3.7) increased risk with dyspnea.
Conversely, older age (HR per decade = 0.45; 95% CI, 0.31-0.67), higher BMI (HR = 0.95; 95% CI, 0.91-0.99) and African American race (HR = 0.41; 95% CI, 0.23-0.74) showed a decreased risk for suicide/overdose mortality in this model.
Mean FEV1 percent predicted was 76.1 ± 25.5 for the total cohort, but researchers noted this measure was not linked to risk for suicide.
Future studies, recommendations for clinicians
The results of this study underscore the importance of incorporating subjective measures of disease symptom severity when assessing suicide/overdose risk among individuals with smoking exposure and COPD, according to Hoth.
“Future studies can be improved by gathering more information about comorbid mental health conditions at baseline so that the impact of depression and anxiety can be included in modeling predicting suicide/overdose,” she said.
Based on the study’s results, clinicians should check adults with a smoking history and heavy symptom burden for depression, anxiety and suicidal ideation, Hoth added.
“Some suggestions for the clinician who is concerned about risk for suicide/overdose for one of their patients include:
approach interactions with patients with a calm, open, curious manner asking about quality of life and things that matter to the patient — a move toward whole-person care has a positive impact;
familiarize themselves with determining level of suicide risk and tools available in their health care setting, with recommendations available in an article by Weber and colleagues in Medical Clinics of North America;
contact family or friends with permission when needed for information and support;
work with the patient or family to reduce access to lethal means (eg, firearms, excess medications); and
facilitate mental health treatment when appropriate, emergently if necessary.”
This study by Hoth and colleagues emphasizes the importance of quitting smoking and implementation of a more specific suicide risk assessment for patients who have a history of smoking, according to an accompanying editorial by Natalie B. V. Riblet, MD, MPH, assistant professor of psychiatry at Dartmouth Institute, and Bradley V. Watts, MD, MPH, associate professor of psychiatry at Dartmouth Geisel School of Medicine.
“The results reiterate the critical need to promote smoking cessation as a strategy to reduce morbidity and death in the population,” Riblet and Watts wrote. “Patients who smoke heavily will also be helped by having access to mental health treatment. Patients with comorbid COPD and depression or anxiety, in particular, can benefit from pulmonary rehabilitation. Suicide risk assessment in this population may also be improved by incorporation into the clinical evaluation specific factors such as current smoking, use of sedatives, and the presence of dyspnea.”
Results of a randomized, double-blind trial showed that hyperbaric oxygen therapy improved cognitive and behavioral function in children experiencing persistent post-concussion syndrome, as published in Scientific Reports.
Amir Hadanny
Amir Hadanny, MD, chief researcher and head of global clinical operations for Aviv Clinics and certified neurosurgeon, hyperbaric physician and chief medical research officer at the Sagol Center, and colleagues said that persistent post-concussion syndrome (PPCS) is commonly seen in children after traumatic brain injury.
Previous studies have shown adults with PPCS benefit from hyperbaric oxygen therapy (HBOT), prompting researchers to study this treatment in children aged 8 to 15 years who experienced mild to moderate TBI 6 months to 10 years prior that resulted in PPCS.
Fifteen children received HBOT daily for 60 days and 10 received sham treatments, according to the study.
Researchers reported significant increases in general cognitive score, memory, executive function, emotional score, behavioral symptoms, global executive composite score and planning/organizing. These outcomes also correlated with significant improvements in brain MRI microstructural changes.
“The study suggests that HBOT improves both cognitive and behavioral function, PPCS symptoms and quality of life in pediatric PPCS patients at the chronic stage, even years after injury,” the authors concluded.
Healio asked lead study author, Hadanny, to describe how HBOT works and the significance of the study results.
Healio: Please explain how HBOT works.
Hadanny: Before HBOT is considered or included in a patient’s personal treatment plan, each candidate goes through a comprehensive physical, psychological and physiological assessment that includes blood tests, advanced brain imaging (MRI scans and SPECT [single-photon emission computerized tomography] scans), fitness and nutritional analysis.
Once approved for the 12-week program, patients go through 2-hour sessions, 5 days a week, in the comfortable, spacious, multiplace hyperbaric oxygen chambers where they are monitored by medical professionals trained for the specialized hyperbaric environment. Each 2-hour treatment is conducted at a specific therapeutic, yet safe, pressure of 2 atmospheres absolute, equal to the pressure found at 33 feet below sea level.
During the session, the patient breathes 100% oxygen through a personal mask in a unique protocol. The inhaled oxygen fluctuates to harness the body’s regeneration processes. While in the multiplace chamber, patients are seated (as if in a first-class airplane cabin) and participate in a purposeful series of brain exercises on Aviv Clinic’s customized digital tablets.
HBOT helps reverse cognitive and physical injuries by increasing the overall oxygen supply to the body and allowing the brain to recover by triggering neuroplasticity. The method of fluctuating oxygen delivery through Aviv’s treatment program triggers the body’s inherent abilities for regeneration and repair. The body senses the relative change in oxygen and triggers a physiological response; this activates HIF-1 alpha, creating the environment for angiogenesis and stimulation of stem cell proliferation.
Studies have shown that this physiological pathway improves cerebral blood flow, brain metabolism and brain microstructure, leading to improved cognitive and physical functions.
Healio: Does this type of technology need to be FDA-approved? If so, is it?
Hadanny: While HBOT is FDA-approved for several conditions, including burns, carbon monoxide toxicity and decompression sickness, it’s not yet approved for post-concussion syndrome.
Our goal is that through more than 10 years of research and the work of other hyperbaric scientists and researchers, our HBOT protocol will be recognized by the FDA as treatment for conditions like post-concussion syndrome. The same protocols used in HBOT clinical trials are duplicated precisely at Aviv Clinic’s Florida-based facility.
Aviv’s approach to HBOT is far safer than the mild-HBOT or monoplace HBOT chambers currently found in many non-health care facilities, which are not monitored by physicians and can be hazardous if not properly maintained or utilized without scientifically proven protocols. Mild-HBOT “beds” or monoplace chambers are not the same state-of-the-art multiplace chambers that are tested, proven and backed by our double-blinded, sham-controlled clinical studies.
Healio: Please describe how the results of this study are significant to the treatment of post-concussion syndrome in children.
Hadanny: This study is significant because not only is it the first trial that evaluates the treatment of persistent post-concussion syndrome in children, but it also is the first to do that using this unique HBOT protocol. The study provides double-blind, high-quality results suggesting the improvement of cognitive and behavioral function.
This is particularly important as it positively impacts children suffering from persistent post-concussion syndrome even years after the initial brain injury. According to the Brain Injury Association of America, about half a million children suffering from a concussion or traumatic brain injury are discharged from emergency departments in the U.S. each year. While the majority recover in the days and weeks following injury, up to 25% endure symptoms for more than 3 months after their injury and are considered in a persistent post-concussive state, although few are diagnosed accurately.
Children suffering from persistent post-concussive syndrome can experience fatigue, anxiety, irritability, headaches, dizziness and difficulty concentrating or processing words. These symptoms are greatly misunderstood and understudied and often misdiagnosed as other behavioral issues.
Current guidelines for treating concussions span only the first 2 weeks of symptoms. Leaving the brain injury untreated puts the child at a significant disadvantage, directly impacts their development into adulthood and can lead to the need for more mental health care in the future.
The findings of our trial showed a significant increase in cognitive, memory and executive function following the HBOT treatment program. The MRI scans showed improvement in brain structure post-treatment.
Healio: How accessible is such treatment to physicians across the country?
Hadanny: Variations of hyperbaric oxygen chambers are widely available to physicians across the country, but the therapy program and protocols provided at Aviv are exclusive. Aviv Clinics offer HBOT at the core of its brain performance program and involve a specialized, comprehensive approach tailored for each patient, including cognitive and physical training and ongoing medical support from experts tracking progress throughout the program.
Unlike other HBOT monoplace chambers, medical professionals join patients inside the suite during every session. In the unlikely scenario that a problem arises, the medical team is available to administer treatment immediately.
Doctors still do not understand why Parkinson’s occurs. However, the disease has been linked to low levels of dopamine and norepinephrineTrusted Source in the body. Additionally, people with certain risk factors, such as ageTrusted Source and past traumatic brain injury, are more likely to develop the condition.
Now researchers from the University of Rochester are adding additional evidence by finding a link between Parkinson’s disease and a commonly-used chemical called trichloroethylene (TCE).
Dr. Ray Dorsey, a professor of neurology at the University of Rochester and lead author of this study, said he and his team decided to research a link between TCE and Parkinson’s disease while preparing to write his book, Ending Parkinson’s Disease.
“One of my colleagues and co-authors of this paper, Dr. Caroline Tanner, told me about TCE and Camp LejeuneTrusted Source,” Dr. Dorsey told Medical News Today. “She and her colleague, Dr. Sam Goldman — another (study) co-author — had conducted a twin studyTrusted Source showing that twins with an occupational or hobby exposure to TCE had a 500% increased risk of Parkinson’s disease. The more I investigated the prevalence of TCE and its role in Parkinson’s disease, the more I (found) with no end in sight.”
For this study, Dr. Dorsey and his team conducted a literature review. They compiled seven case studies of individuals who developed Parkinson’s disease after exposure to the chemical from either the workplace or the environment.
The case studies include NBA player Brian Grant who received a Parkinson’s diagnosis at the age of 36. According to researchers, he was likely exposed to TCE as a child when his father was stationed at Camp Lejeune in North Carolina.
The camp’s water-supply systems were found to be contaminatedTrusted Source with TCE in the early 1980s.
The researchers also profiled a Navy captain who had served at Camp Lejeune and was diagnosed with Parkinson’s 30 years after.
And the research team also spotlighted the late United States Senator Johnny Isakson, who served in the Georgia Air National Guard, which used TCE to degrease airplanes. Senator Isakson was diagnosed with Parkinson’s disease in 2015.
“Currently, the world’s literature on trichloroethylene and Parkinson’s disease is limited to 26 studies based on a search on PubMed,” Dr. Dorsey said. “Given the widespread use and pollution with TCE and perchloroethyleneTrusted Source (PCE), widely used in dry cleaning, and the rise of Parkinson’s disease, more research is needed. We call for that.”
“The seven individuals add to the existing literature — the largest previous case series was three — and demonstrate the myriad of ways that individuals can be exposed to the chemical via work or the environment,” he added. “Importantly, most are unaware because they never knew about the exposure and it occurred decades ago.”
In order for people to lower their exposure to TCE, Dr. Dorsey stated at a societal level the U.S. should ban TCE and PCE.
“In January 2023, the EPA found that TCE ‘poses an unreasonable risk to human health’,” he continued. “A month earlier, it concluded the same about PCE. We don’t drive cars or fly airplanes from the 1920s, when commercial production of TCE began, because engineers have developed safer alternatives. Chemists can do the same.”
“Second, we should notify the public, especially those who live near contaminated sites, contain them, and prevent the entry of these gases into homes, schools, and workplaces with relatively inexpensive remediation systems, akin to what is used for radon,” Dr. Dorsey added.
MNT also spoke with Dr. Ariana Spentzos, Ph.D., Science and Policy Fellow at the Green Science Policy Institute, who was not involved in this study.
Dr. Spentzos said it is unsurprising that this study found a link between TCE exposure and Parkinson’s disease. She explained:
“TCE has a number of known adverse health effects and several studies over the last few decades have suggested TCE exposure as a risk factor for Parkinson’s disease even from exposures decades before disease onset. The Department of Labor has even issued guidance on workers’ compensation acknowledging a link between TCE exposure and Parkinson’s.”
For people looking to lessen their TCE exposure, Dr. Spentzos said most TCE exposure occurs through inhalation.
“Indoor air qualityTrusted Source can be improved by increasing ventilation or using air filtersTrusted Source with activated carbon, although more sophisticated systems used for radon mitigationTrusted Source are most recommended,” she detailed. “Since up to 30% of drinking water in the U.S. may be contaminated with TCE, the easiest way to reduce TCE levels is to filter your drinking water with activated carbon filters. Whole-house water filter systems can help avoid additional exposure through bathing, dishwashing, or other household uses.”
“Additionally, avoid using any TCE-containing consumer products,” Dr. Spentzos added. “Check to make sure that any paint strippers, stain-removers, adhesives, degreasers, and sealants, among other products, do not contain TCE in the ingredients list.”
Acupuncture and chiropractic care weren’t always the common fixtures of employer benefit plans they are today. It took clamoring from workers, the accumulation of evidence, and the slow realization by businesses that those perks would be popular with workers.
A similar evolution could be in store for psychedelic-assisted therapy for mental health conditions. Health insurers are years away from covering the interventions, but employers — eager to offer whatever perks might entice talent — may be poised to do so much sooner. And now, a Boston-based startup called Enthea wants to speed up the adoption of this benefit by self-insured employers — though data to support the effectiveness and safety of these treatments are still limited.
“Employers will add things to what they offer employees based upon what they hear their employees saying they want, especially in competitive job markets like we have right now,” said Paul Fronstin, director of health benefits research at the Employee Benefit Research Institute. “So in some respects, this fits in.”
Even as ketamine clinics proliferate for the treatment of conditions like depression and post-traumatic stress disorder, their use is largely restricted to people with the means to shell out thousands of dollars. Enthea is hoping to make psychedelic-assisted therapy more broadly available.
“There are still no standards of treatment and there’s still no way to create access,” said Sherry Rais, Enthea’s CEO and co-founder. “That’s why Enthea is bridging these gaps. There’s so much I’m excited about.”
Enthea is a third-party administrator that charges businesses for access to its list of vetted providers, plan designs, and clinical policies. The company got a lot of attention earlier this year when it signed the soap company Dr. Bronner’s, which supports psychedelic initiatives including the ballot measure for legal magic mushrooms in Colorado, as its first customer. But despite the high-profile client, Rais said the small, not-for-profit operation “ran out of money” not long after and shut its doors to new customers until it could turn things around.
Now, refueled with $2 million in seed funding and retooled as a public benefit corporation, Enthea is announcing an ambitious expansion: The company plans to enter 40 markets, sign 100 new customers, and add 80 ketamine providers to its network by the end of next year.
Psychedelic-assisted therapy is currently limited to ketamine and its chemical mirror, esketamine, as these are the only such drugs approved by the U.S. Food and Drug Administration. Esketamine, which was created by Johnson & Johnson, is the only psychedelic approved for treatment of depression, while ketamine has FDA clearance as an anesthetic and is used off-label as a mental health treatment.
When it comes to prescription drugs, sometimes the off-label use is more common than the on-label one, said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms. In those cases, it’s up to the health plan or employer to decide whether they want to cover the off-label use.
“There may be market demand and insurers feel like they have to offer it to maintain competitiveness,” she said.
Not everyone agrees focusing on individual employers is the best way to expand access to psychedelic-assisted therapy. Compass Pathways, a mental health company with the most advanced clinical trials on psilocybin for treatment-resistant depression, shares Enthea’s goal of expanding access, but it’s taking a different approach: traditional insurance coverage.
To that end, Compass and MAPS Public Benefit Corporation, the organization behind the most advanced trials on MDMA, recently submitted an application to the American Medical Association for a current procedural terminology code for psychedelic therapy that accounts for the lengthy, 6- to 8-hour treatment sessions. CPT codes allow providers to bill insurers for services.
“If there’s going to be broad and equitable access, the route for that is payers,” said Steve Levine, Compass’ senior vice president of patient access. “This needs to be covered through insurance.” He said broad coverage was more efficient: “Outside of that, you’re going one by one and selecting for a rarified group of payers.”
There’s no formal licensing or accreditation program for ketamine providers. The dozens of ketamine clinics in operation vary widely in how thoroughly they screen patients, leading some experts to worry they’re offering the drug to anyone who can afford it, a 2018 STAT investigation found. In many cases, STAT found clinics didn’t have psychiatrists or other mental health professionals on staff, even though they’re working with patients who may have had suicidal thoughts.
That’s why Rais maintains the most important service Enthea offers employers is its credentialing process. The company examines several aspects of providers’ operations to ensure safety, including where they were trained, what licenses they have, how long they’ve been providing services, whether they have malpractice insurance, and whether they’re under investigation.
“We kind of take a holistic look at their business and then we can credential them,” she said.
Right now, Enthea has just one provider in its network, Flow Integrative, the company that Dr. Bronner’s uses. But it has received letters of interest from more than 90 providers in 26 states and is busy working through the list to credential them. In January, the company will launch services in New York City, Austin, Texas, and the San Francisco Bay Area.
On the customer front, Enthea has received interest from 32 employers spanning a range of industries, including personal wellness, food, software, and even finance. The company says it’s also signed a handful of new clients, including Tushy, which makes bidets, and Daybreaker, a company that hosts sober morning dance parties.
“The commonality is they, I hope, care about the wellbeing of their employees and want to do something to help their employees’ mental health, and just that says a lot,” Rais said.
Once employers decide to offer the therapy as a benefit, employees can search the list of nearby in-network providers. The provider they pick assesses them and sends the information to Enthea, which determines if the patient is eligible for treatment. Though ketamine hasn’t been approved by the FDA for any mental health condition, Enthea authorizes ketamine treatment for eight conditions, though Rais said employers can narrow that list. The conditions include treatment-resistant depression, major depressive disorder, bipolar disorder, PTSD, generalized anxiety disorder, social anxiety disorder, substance use disorder, and adjustment disorder.
Esketamine has been approved only for treatment of depression.
One safety concern with use of psychedelics for unapproved conditions is that the vast majority of clinical trials of psychedelics exclude participants with a risk of psychosis — including those who have a relative with bipolar disorder or schizophrenia — out of fear that psychedelics could trigger psychosis.
“Ketamine and bipolar is a potentially dangerous combination,” said Boris Heifets, a neuroscience researcher at Stanford University who studies psychedelics. “I don’t think it’s well enough researched to administer ketamine to bipolar patients, especially someone who recently had a manic episode.”
The lack of data around the connection to psychosis makes treatment of bipolar disorder with ketamine particularly uncertain; of the studies that exist, some try to minimize the likelihood of a switch to mania by requiring participants to be on a mood stabilizer. A 2021 review of psychedelic literature identified 17 cases of adverse events that seemed to involve mania, and researchers last year found high-dose ketamine triggered hypomania in at least one participant with a bipolar II diagnosis.
Rais said Enthea includes bipolar disorder among its covered conditions because research suggests ketamine-assisted therapy can be “quite effective” during the condition’s depressive phase. She said the company would discuss possible risks with the prescribing clinician before treatment and “would not authorize treatment for patients where we believed there was risk of mania or psychosis.”
Ketamine treatments cost an average of $8,000 among the providers Enthea has spoken with, Rais said. That includes medical and psychiatric evaluations, one to three prep sessions, four to six medication sessions, and six to eight integration sessions, which refers to therapy to process the ketamine experiences.
Employers decide for themselves how much of the treatment they want to cover versus how much workers cover. Dr. Bronner’s, for example, is covering 100% of the treatment cost, but others might choose to cover 75%, Rais said. Enthea charges an 8% fee for its services.
Enthea says it plans to expand to other psychedelics, including MDMA and psilocybin, if those become FDA-approved.
Marik Hazan, managing partner with Tabula Rasa Ventures, the psychedelic-focused venture capital firm that led Enthea’s seed fund raise, agrees securing insurance coverage is crucial, but he thinks Enthea’s approach of starting with employers is an important first step. It’ll allow the company to collect data on how well the therapy works and whether it’s cost-effective.
“It’s hard for me to imagine an opportunity that will be as impactful to people’s abilities to access psychedelic therapy in the future than a company like Enthea,” Hazan said.
Realistically, a relatively small number of people will benefit from what Enthea’s offering, said Elliot Marseille, director of the University of California, Berkeley’s Global Initiative for Psychedelic Science Economics. His research has found MDMA treatments for PTSD patients could save health insurers millions of dollars, mostly because chronic medical conditions like diabetes and cardiovascular disease tend to improve as PTSD improves.
Natalie Gukasyan, a psychiatrist and post-doctoral research fellow at Johns Hopkins University who’s researching the feasibility and efficacy of psilocybin-assisted psychotherapy, agreed that this kind of insurance plan seems unlikely to be widely used.
“Who’s going to sign up for a super specialized insurance company, apart from people who think they need a lot of psychedelic therapy?” she said.
A woman demonstrates what a patient would experience in a therapy room at Field Trip, a psychedelic therapy clinic in Toronto.
Psychedelics like psilocybin and ketamine are being touted as the next generation of treatment for depression, anxiety, and other mental health issues. There’s no question that a next generation is needed. But it’s not like flipping a switch: These therapies involve a novel administration paradigm, acceptance by regulatory bodies, and public appreciation of their unique medicinal value.
The most common first-line treatments for depression, selective serotonin reuptake inhibitors (SSRIs) like Prozac, were introduced nearly a half century ago. While these medicines have had a major impact on treating depression, SSRIs do not work for around 30% of people with major depressive disorder. And even when they are effective, it can take several weeks for them to begin working, and they must be taken continuously for years. Side effects and adverse events like dry mouth, nausea, weight gain, and sexual dysfunction cause people to stop taking them, take them infrequently, and/or switch from one to another in search of improved effectiveness or tolerability.
The advent of psychedelic therapies
Problems with SSRIs led to a revival of research into the mental health benefits of psychedelics that began in the early 1990s, after a 25-year hiatus due to the war on drugs and related prohibitive drug scheduling of psychedelics. Thirty years later, the field is past the “early promise” stage. Johns Hopkins University in Baltimore, the University of California, Berkeley, and the Icahn School of Medicine at Mount Sinai in New York City, among others, have opened centers devoted to studying psychedelics for mental health.
There’s growing scientific consensus regarding the therapeutic potential of psychedelic drugs, and regulatory agencies are beginning to accept how psychedelics treat depression and other mental issues. But it will take some doing to make these therapies ready for prime time. For one thing, it will be essential to develop psychedelic therapies with psychoactive states lasting less than four hours, something my company, Reunion Neuroscience, and others are working toward.
Unlike taking a simple SSRI pill, psychedelic therapies require three distinct stages: preparation, the session, and integration.
In the preparation stage, the clinician must establish trust with the patient and reassure them that the treatment will be safe and effective. Being able to reassure a patient, especially one who has never before had a psychedelic experience, that the psychoactive state is short should serve to ease anxieties and lead to a better overall experience.
During the session, a shorter psychoactive state is useful from a practical point of view. If a psychedelic experience lasts up to eight hours, two trained monitors must be available the entire time. But there’s a limit to how many trained monitors are available — at double the cost — so the possibility of needing only half as many monitors opens the door to treating more patients.
After the session, psychological support is used to help the patient reflect on the insights gained during the psychedelic experience, unpacking them for ongoing use. This is distinct from psychotherapy, because it’s limited to a short time immediately after the session.
In addition to the details of providing psychedelic therapy, another real challenge is the need for stronger intellectual property for psychedelic products. Many of these are currently generic products, which may limit companies from broadly investing in clinical development and commercialization. As a result, companies may find they lack the financial strength to help overcome the inevitable barriers to widespread adoption.
Another thing to consider is how traditional behavioral psychotherapy will interact with psychedelic treatment. It will require collaborative efforts to creatively integrate a new paradigm of administering these products to patients with chronic depression and anxiety. While more research is needed on the durability of psychedelic therapies, depending on the disease state there’s a possibility that a single-dose treatment may be sufficient to provide long-term symptom control, particularly in areas where the mental health condition is acute, like postpartum depression.
I believe that passion and staying power will both be needed: the right kind of stubbornness and the right kind of resources to fund the right kind of teams.
Let’s make the second age of psychedelic therapies a reality.
Although many view a colonoscopy as an uncomfortable or even scary procedure, around 15 million of them are carried out annually in the United States, and 60.6 percent of people aged 50 to 75 without a personal history of colorectal cancer have had one in the past 10 years.
It’s believed that a colonoscopy not only helps find cancer but also prevents cancer from developing from polyps. Because of its high level of sensitivity and specificity, colonoscopies have been regarded as the gold standard for colon cancer screenings for a long time.
Unexpected Result From a Major Colonoscopy Study
However, a recent major clinical study, the Nordic-European Initiative on Colorectal Cancer (NordICC) study published in October 2022, raised questions about the efficacy of colonoscopies.
The study suggested that colonoscopies don’t save as many lives as previously thought.
Researchers recruited 84,585 participants in Poland, Norway, Sweden, and the Netherlands; 28,220 were in the invited group (invited to have a colonoscopy), and 56,365 were in the usual-care group.
At the end of the 10-year follow-up, the risk of colorectal cancer-related death at 10 years was 0.28 percent among participants in the invited group and 0.31 percent in the usual-care group. The risk of death from any cause was 11.03 percent in the invited group and 11.04 percent in the usual-care group.
In terms of adverse events, 15 people had major bleeding after polyp removal. According to the study, there were no screen-related deaths within 30 days after colonoscopy.
The incidence of colon cancer has dropped significantly since 1975. Most people believe that this is due to increased screening and improved treatment.
Since there were no randomized clinical trial data on colonoscopies for colorectal cancer before, the NordICC trial sparked a heated discussion: Can colonoscopies truly prevent colon cancer?
If the benefit isn’t what people have expected, the colon cancer-screening landscape could be totally reshaped.
Numerous doctors argue that NordICC’s researchers should maintain follow-up in their study, and assessments of other current trials may shed light on the advantages of screening colonoscopies after 10 years. Follow-up time is very important, as many believe that the benefit of a colonoscopy is treating precancerous polyps. It may be decades before we see the long-term benefit of colonoscopy screenings.
Doctors perceive the results of the NordICC study differently for the following reasons.
First, the trial had lower-than-expected participation—only 42 percent underwent colonoscopy—and provides no information on adherence to guidelines for polyp surveillance.
Most think the study doesn’t change the value of colonoscopies. The test would’ve lowered cancer risk by 31 percent and cut the probability of dying from colorectal cancer by 50 percent if compliance had been 100 percent, according to the research findings.
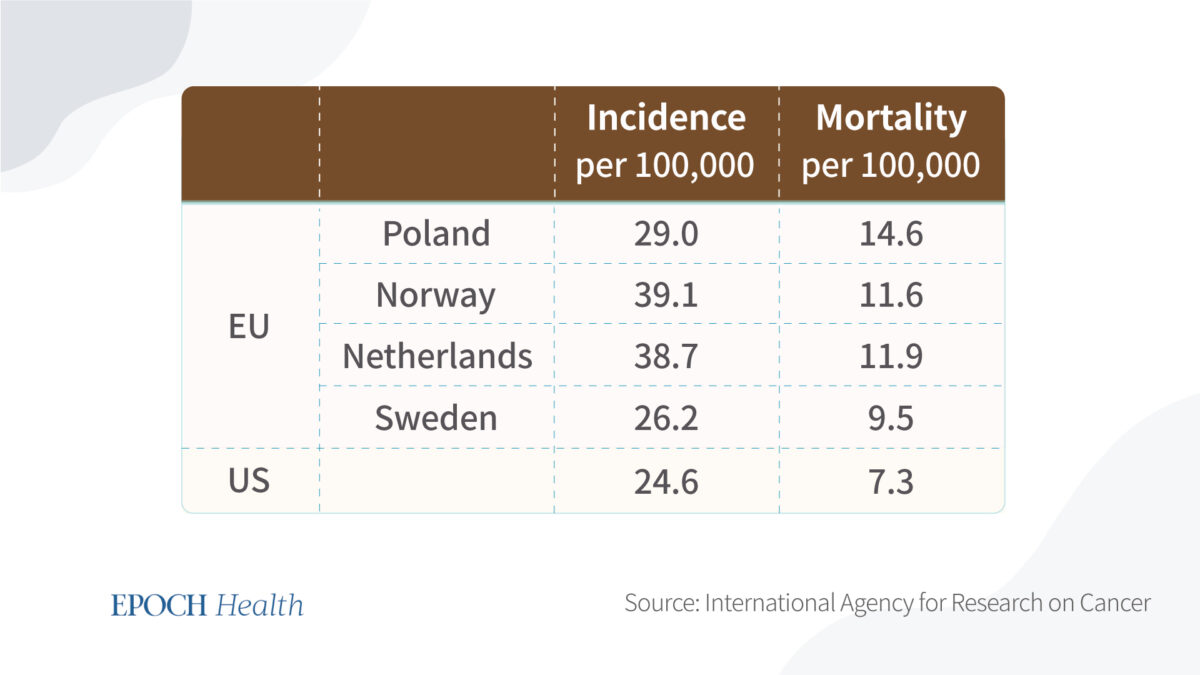
Also, the tested countries have a higher mortality rate and incidence rate compared to the United States. U.S. clinicians favor colonoscopies, while European health systems rely far more on flexible sigmoidoscopy, which only examines the lower part of the colon.
Comparison in incidence and mortality of colorectal cancer in the United States versus Europe, 2020. (The Epoch Times)
However, countries without screening programs still witnessed improvements in colorectal cancer mortality. A comment on the findings published in The Lancet Oncology stated that firm conclusions can’t yet be drawn on the causal relationship between colon cancer mortality and national screenings.
Second, the operator affects the colonoscopy’s effectiveness. The adenoma detection rate is the percentage of screening colonoscopies in which one or more adenomas are found.
Patients are better protected from adenoma development by endoscopists with higher adenoma detection rates.
Third, the study was done among European populations and may not be representative of the various demographics in the United States.
The Risks of Colonoscopy
The benefits and risks depend on compliance with the screening protocol, the chance of meeting with an experienced endoscopist, and your own risk of developing colon cancer.
For a person with a family history of colorectal cancer, it might be more beneficial to keep a close look and a healthy diet.
On the other hand, a healthy lifestyle doesn’t guarantee that you won’t have colorectal cancer. First-degree relatives of people with colorectal cancer are at a sixfold increased risk of colon cancer before 50 years old. Second- and third-degree relatives correspond to 1 1/2 and three times increased risk, a two- to threefold increased risk of colorectal cancer.
A doctor may determine that you’re at high risk if you have a family history of colon cancer or you have a history of colon polyps or inflammatory bowel disease.
Colonoscopies are still the gold standard if cancer is suspected in a patient. And it will benefit patients most if a cancer is found and removed in the adenoma-carcinoma sequence (the development of cancerous change in a dysplastic polypoid lesion).
The prognosis of patients with colorectal cancer varies according to the site of cancer, with right-sided tumors having the most severe prognosis, making an early diagnosis in this group of patients especially important.
However, there are many risks for colonoscopies—in addition to the risk of sedation.
The risks of colonoscopies include major bleeding (14.6 events per 10,000 performed), perforation (3.1 per 10,000), or infection. These rates are higher than in sigmoidoscopy, a less expensive, less invasive method that can be performed without sedation.
A colonoscopy is more invasive and burdensome than other colon cancer tests, such as fecal testing and sigmoidoscopy, and it requires more clinical resources.
A few medical organizations have dropped the recommended age to begin colorectal cancer screening to 45 from 50. The reason for this is that scientists are striving to learn more about the causes, the biology, and how to prevent the illness from developing earlier in life. Several risk factors have become more prevalent over the past 45 years, such as obesity, sedentary lifestyles, and smoking, which can lead to more instances of early-onset cancers. Poor diet, particularly one high in processed meat and fat and low in fruits and vegetables, is increasingly being linked to early-onset colorectal cancer. Several studies have also discovered that being overweight or obese may increase one’s risk of developing colorectal cancer with early onset.
Since colorectal cancer is still relatively rare, affecting less than 1.8 per 100,000 younger adults (below age 40), lowering the screening age might be a burden and not cost-effective. In addition, the trend of new young patients might be because of early screening and overdiagnosis, which could further burden the person.
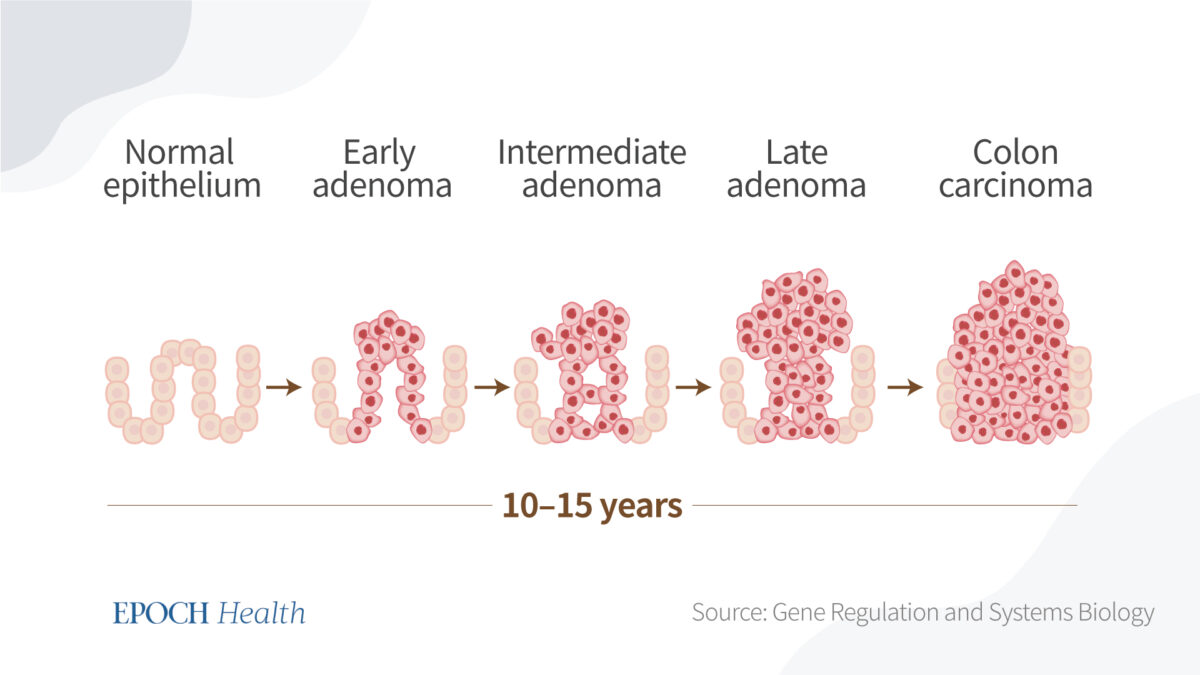
The below figure shows the long process of colon cancer development. If the in situ cancer is identified very early, the five-year survival rate may improve. But no one can really tell how long it takes for a cancer cell to grow into something lethal, and there are other risks to consider that may affect outcomes, as well.
It takes 10–15 years for colon carcinoma to form. (The Epoch Times)
Weigh Both Sides
Deciding whether it’s cost-effective to do a colonoscopy will be based on your own risk of developing colorectal cancer, depending on your family history and other risk factors.
If you develop severe bleeding due to receiving an endoscopy, harm is 100 percent likely. To avoid the chance of harm, or if you can’t tolerate a colonoscopy, some studies have proven that a fecal immunochemical test for screening patients at increased risk for colorectal cancer has high overall diagnostic accuracy, given its safety, simplicity, low cost, accuracy, and minimal discomfort.
We still need better data on a colonoscopy’s benefits and risks. To account for comorbidities, oncological treatments, stage-related differences at the time of diagnosis, family history, and other risk factors, additional in-depth patient-level data are required.
Ideally, when a patient sees a doctor, the doctor would provide him personalized advice; for example, “Mr. Smith, your chance of getting colorectal cancer is X percent based on all the information you’ve provided.”
However, there are many uncertainties in life. Even in the way you cook, what ingredients you use, and how they were processed—it’s hard to digitize such factors, as there’s no single model to predict a person’s risk. Tailoring colorectal cancer screening approaches to each person based on their risk factors and precision screening may improve the efficiency and cost-effectiveness of colonoscopy screening.
Scientists will need to carry out in vivo tests on animals before thinking about doing human trials. They estimate that the bot will be ready for clinical use in five to seven years if all goes according to plan.
Australian researchers have invented a snake-like soft robot, designed to 3D print living cells from the inside of patients’ bodies. This development may soon eliminate the need for invasive surgeries to transplant 3D printed tissues and treatments, reported Freethink.
What are 3D bioprinters?
Similar to conventional 3D printers, 3D bioprinters build three-dimensional objects by layering ink. The only distinction is that they employ bioinks that contain living cells in them.
Researchers are using 3D bioprinters to produce ear implants for children who were born with birth abnormalities, stem cell patches to treat babies’ hearts, and cartilage for reconstructive rhinoplasty.
3D bioprinting makes it seamless to create tissues in precisely the shape and size required. Considering a patients’ own cells can be used in the ink, the risk of rejection is lowered.
However, there is still a need for invasive implantation surgeries, which bioprinting cannot yet replace.
“Current 3D bioprinting techniques need the creation of biomaterials outside the body, and implanting those into a human would often require big open-field surgical surgery, which increases the risk of infection,” said Thanh Nho Do, a biomedical engineer at UNSW Sydney who spoke to Freethink.
How do 3D bioprinters function?
Aside from printing bioinks, the soft robot can function as an endoscope, electric scalpel, and water dispenser. Researchers have tested these functions in an artificial colon and a pig’s intestine and kidney.
Before considering human trials, scientists will have to conduct in vivo testing on animals. If everything goes as planned, they anticipate that the bot will be ready for clinical use in five to seven years.
Once put into the colon, the robot may remove a difficult-to-reach tumour and then 3D bioprint material to promote healing on-site. If the robot passes development, clinicians may be able to use it to treat colorectal cancer, which is the second most common cause of cancer deaths, reported Freethink.
Cancer is a type of disease in which some abnormal or damaged cells of the human body grow uncontrollably, multiply, and spread. These cells may form lumps of tissue called tumors, and in the case of cancerous (malignant) tumors, they travel to other parts of the body to form new tumors.
The first ever documented case of cancer took place in ancient Egypt in 1500 B.C. It’s possible that humans’ fight against cancer is as long as the history of human civilization itself. Despite generations of efforts, thousands of years have passed, and we still haven’t found a cure for cancer.
However, new medical and scientific discoveries and developments might bring about new treatment methods to prevent or eliminate cancer. For instance, scientists may have discovered a way to prevent at least half of all cancer cases.
Discovery of a Key Trigger of Cancer
In 2019, in an interview with the Horizon magazine, virologist and Nobel laureate Professor Harald zur Hausen, winner of the 2008 Nobel Prize in Physiology or Medicine for his discovery of the role of papilloma viruses, stated that humans have a good chance of drastically reducing the incidence of cancers.
He further explained that according to our current understanding of different types of cancer, in about 20 percent of cancer cases, infections are involved.
According to Professor zur Hausen, there’s evidence that at least 30 percent more human cancers are also linked to infectious events. Therefore, by eliminating infections, at least half of the human cancers can be prevented.
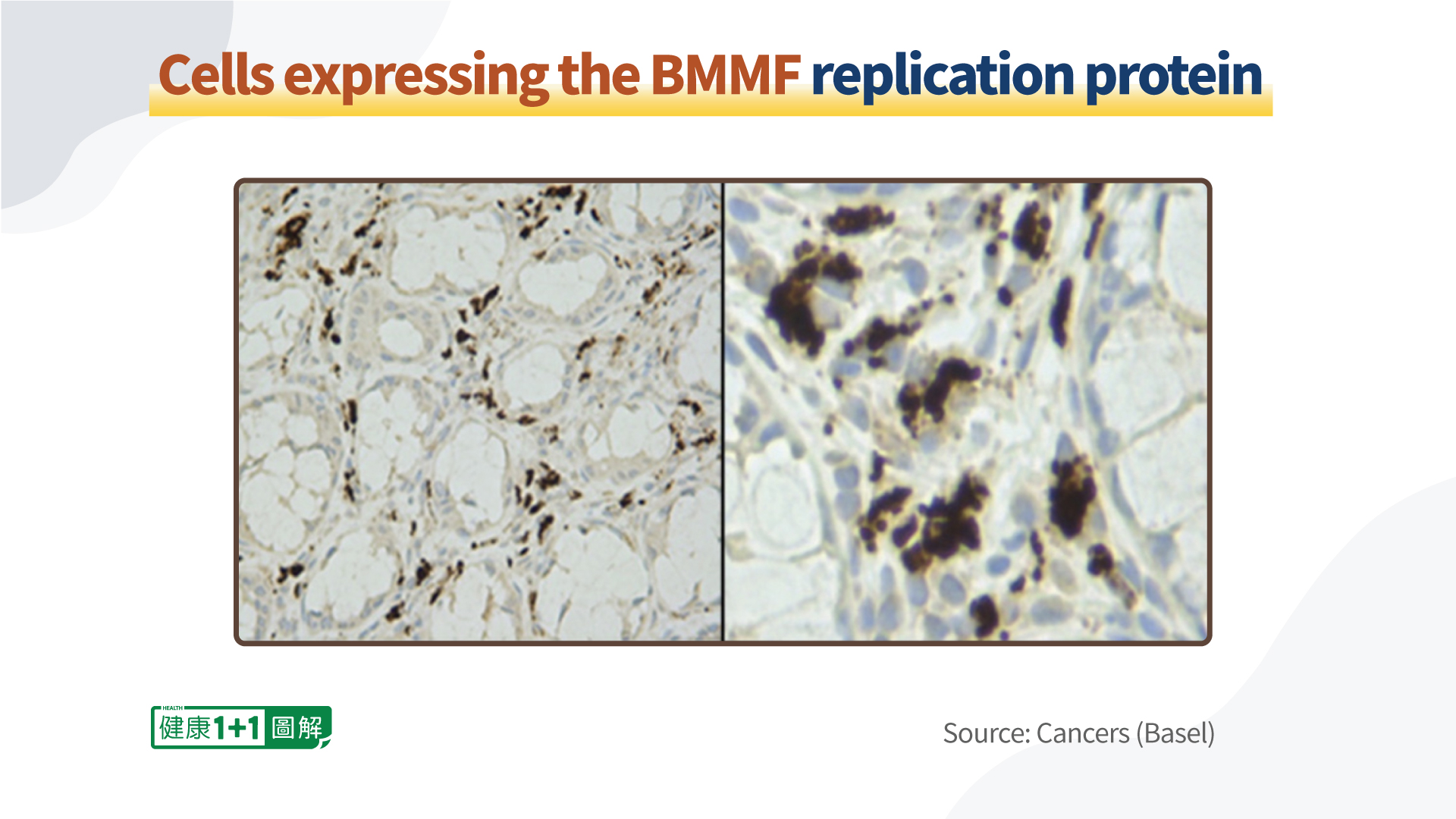
Just several years ago, in 2015, Professor zur Hausen and his wife Professor Ethel-Michele de Villiers, who both worked at the German Cancer Research Center, discovered a new form of infectious agents called “Bovine Meat and Milk Factors” (BMMFs) in dairy products and bovine sera. These BMMFs are active in human cells, and replicate and produce proteins.
The Cancers Related to Infections
Some types of human cancer are caused by viral, bacterial, or parasitic infections, which are causative agents in this regard. For instance, Hepatitis B and C virus infections may cause liver cancer; Helicobacter pylori infections may lead to ulcers and possibly gastric cancer; parasitic infections of the vascular system in the bladder and liver may eventually lead to bladder and liver cancers; and HPV infections may lead to cervical cancer.
According to the calculations performed by de Villiers’s team, the global cancer incidence caused by infections is somewhere between 20 percent and 21 percent.
Infectious agents contribute to cancers by both direct and indirect interactions. The cancers induced by direct carcinogens (e.g. papilloma viruses, EBV, and retroviruses) differ from those induced by indirect carcinogens (e.g. Helicobacter pylori and parasitic infections). Cancers linked to direct carcinogens commonly increase under immunosuppression, whereas the cancer risk by indirect carcinogens would decrease. The group of cancers induced by indirect carcinogens include colon, breast, and prostate cancers.
What Are Bovine Meat and Milk Factors (BMMFs)?
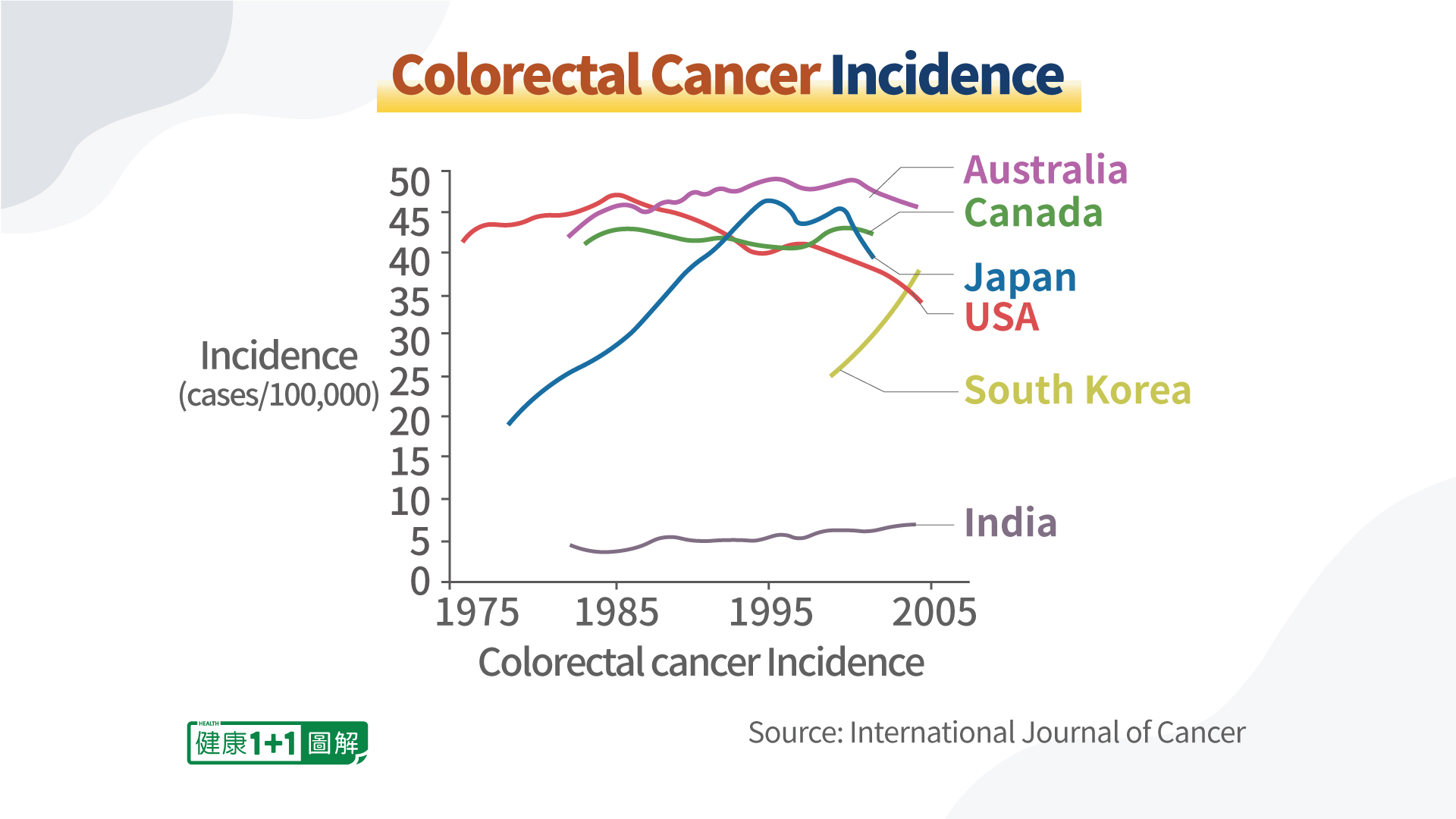
By analyzing epidemiological data, Professors zur Hausen and de Villiers and their team have discovered a link between the consumption of dairy cattle’s meat and milk and several types of cancer. Specifically, it was found that countries consuming red meat mostly from Eurasian dairy cattle origins have high incidences of breast and colon cancers, with the exception of Mongolia.
The team’s studies in Mongolia support the suspicion that species-specific factors should be more important, possibly linked to specific breeds of cattle.
Cow milk (bovine milk) and beef (bovine meat) have always been an important part of human diet, and they have brought undoubted health benefits to the human race for millennia. Besides the obvious negative effects of lactose intolerance and dairy allergy, scientists have also identified more than 100 different types of viruses or infectious DNA molecules in bovine meat and milk that can potentially cause human cancers. And they are called the “Bovine Meat and Milk Factors” (BMMFs).
BMMFs can be found in beef, milk, and other dairy products, including butter, yogurt, yogurt drinks, and cheese.
They share characteristics with viruses and bacterial plasmids
They are adapted to genetic activity and replication in certain cattle and human cells
The majority of the initial isolates originated from sera or dairy products of Eurasian dairy cattle
Their DNA doesn’t persist in cancer cells, but it stays in lamina propria cells (including periglandular stroma cells and in some macrophages)
They produce a protein product called Rep, which can multiply in cells
BMMFs are biologically active in human cells and are proposed to induce chronic inflammation (proven to promote cancers) in precancerous tissues, which leads to increased free radical (reactive oxygen species) formation and increased mutagenesis at the respective sites.
Colon, Breast, and Prostate Cancers
According to the American Cancer Society, as of 2022, colorectal cancer (colon cancer for short) is the third leading cause of cancer-related deaths in both American men and in women.
According to epidemiological evidence, not every cattle species’ beef and milk can lead to colon cancer. For example, consumption of Zebu (from humped cattle) and Yak meat seems to be able to substantially reduce the risk of colon cancer. This may explain the low incidence of colon cancer in Mongolia.
On the contrary, the consumption of meat and milk from dairy cattle (Eurasian taurines) seems to increase the risk for colon cancer, because in countries with high incidences of this cancer, dairy cattle are the most prevalent. A current working hypothesis is that Eurasian dairy cattle might carry and transmit a factor that’s involved in colon cancer etiology. This factor is an infectious agent that contributes to malignant conversion of colon cells, due to the selective expression of growth-stimulating genes.
The BMMFs can enter and multiply in human cells.
It has been discovered that they can infect humans at an early age and start accumulating in the colon’s immune cells. Consumption of BMMF-containing beef and milk over a long period of time will lead to chronic inflammation in the colon. Lamina propria cells (stromal mesenchymal cells and CD68-positive macrophages) will be infected by these agents, which will lead to macrophage-mediated inflammatory responses (i.e. reactive oxygen production).
With BMMF accumulation, the immune cells become weakened, so they can no longer effectively defend against infections.
Some cells in the colon may develop into tissue antecedents of cancer. Random mutagenesis in DNA-replicating intestinal gland (crypt) cells, which are adjacent to infected cells, and in replicating single-stranded BMMF-DNA will take place. After an incubation period typically longer than three decades, “driver” mutations in specific cellular genes are established, and the growth of these clones is enhanced. After further mutations, these clones will lead to the development of precancerous polyps. And as a result of continuing mutagenic activity, these polyps eventually transform into malignant tumors.
In this way, BMMFs contribute to the development of colorectal cancer, with the time of onset generally being 40 to 70 years after a person is first infected with BMMFs.
BMMFs May Induce Breast Cancer
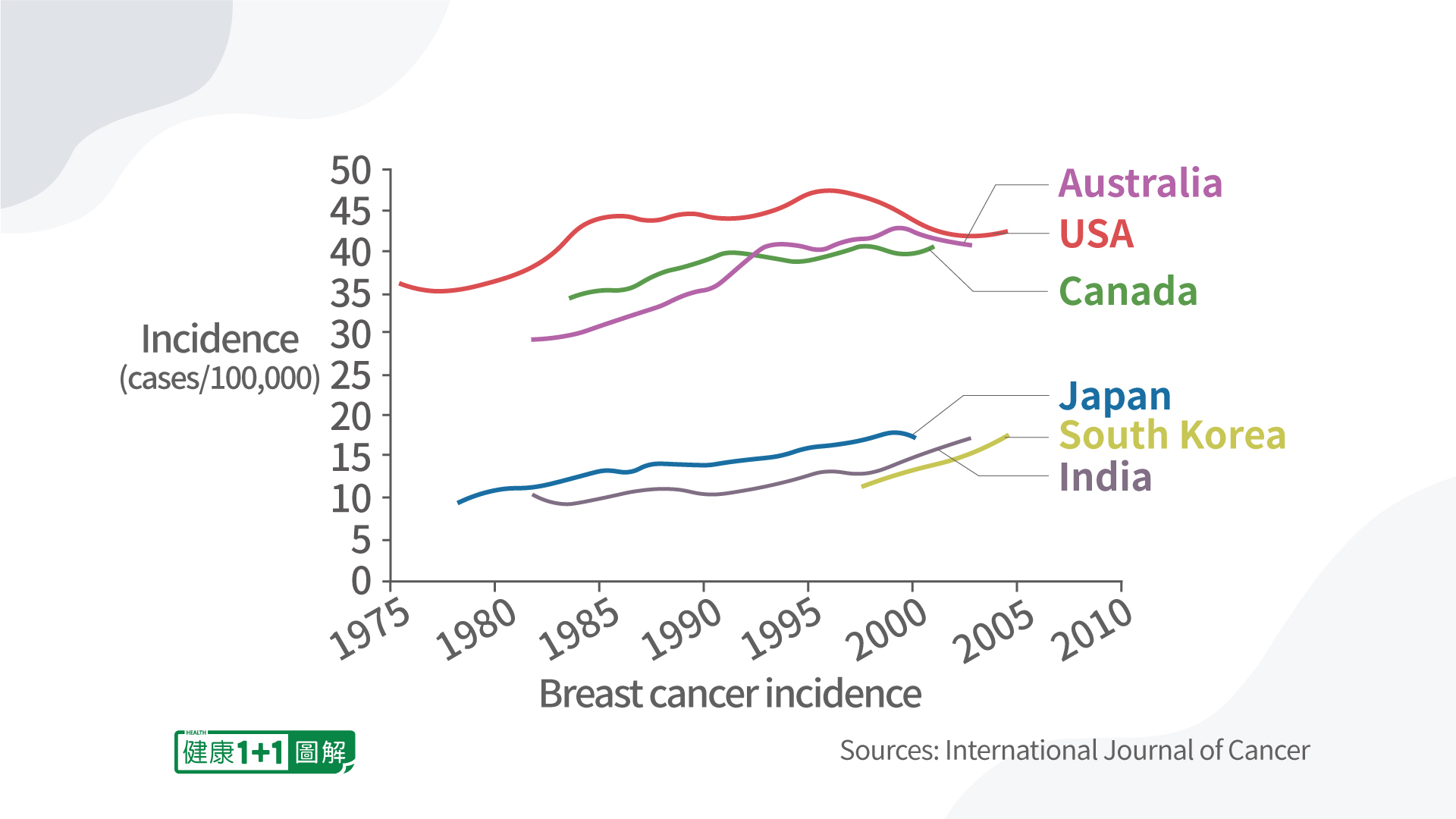
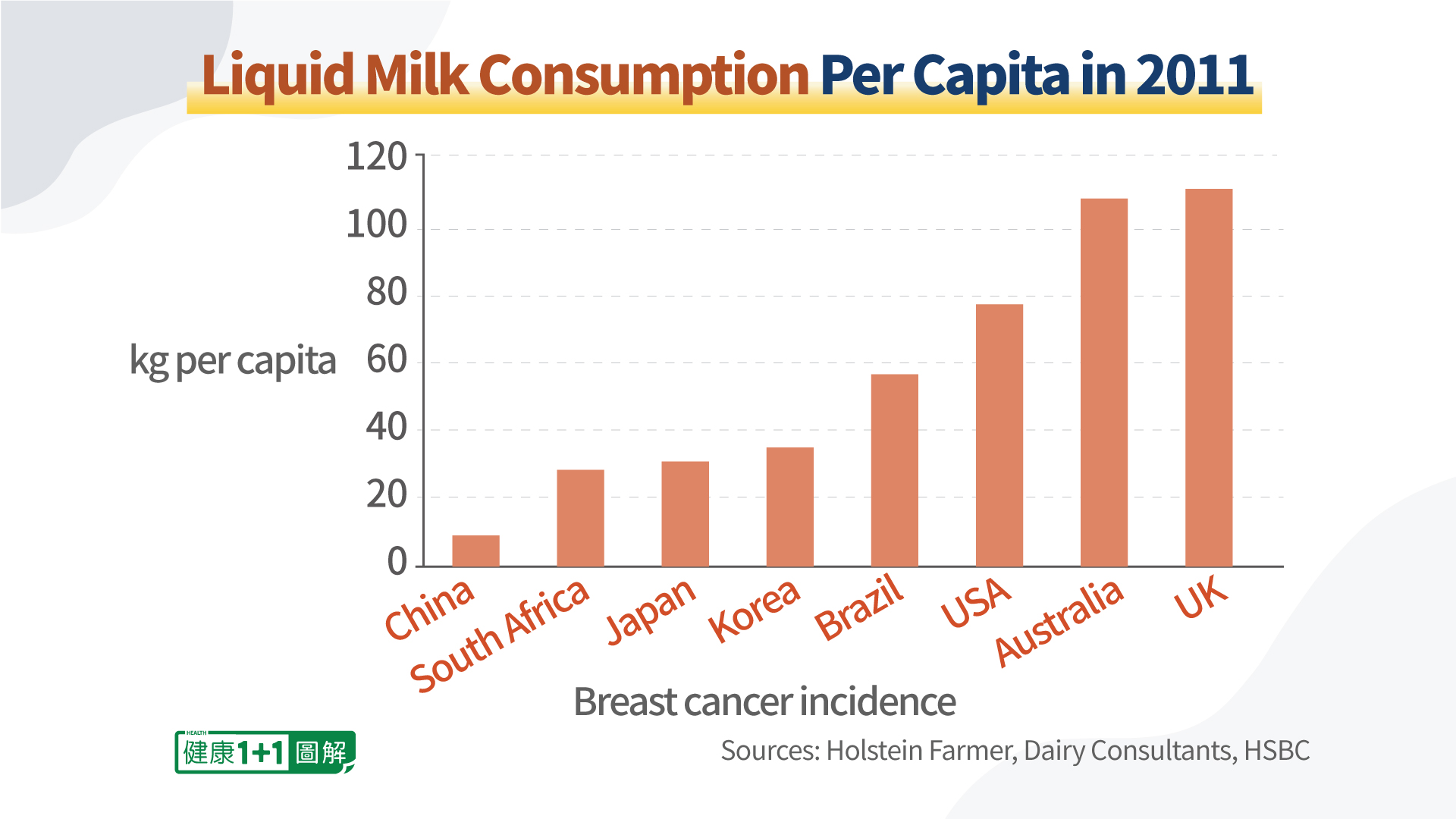
In 2020, female breast cancer became the most commonly diagnosed cancer worldwide. And in the United States, breast cancer is the second most common cancer for women, accounting for one in three new cases annually. The high risk regions for breast cancer are North America, most European countries, Australia, and Argentina. And the low risk regions include India, Mongolia, and Bolivia (which is bordering Argentina). The possible reasons might include that Mongolians primarily consume sheep and goat meat, instead of beef; that India has a relatively low beef consumption, due to religious reasons; and that the milk consumption in Bolivia is among the lowest in the world.
A population-based study published in the British Journal of Cancer showed that individuals with lactose intolerance have reduced breast cancer rates. Lactose intolerance takes place when a person’s body cannot break down or digest lactose, resulting in diarrhea, bloating, and other uncomfortable symptoms. It is caused by genetic modifications resulting in lactase deficiency.
Professors zur Hausen and de Villiers proposed a potential relationship of milk-borne infectious agents to breast cancer. It is speculated that infectious agents in milk have a relatively high affinity to cells of mammals. People’s consumption of milk and dairy products from cows (Eurasian dairy cattle), especially at an early age, is suggested to be one of the main risk factors of breast cancer in their later life.
Cow Milk Versus Other Milk
Certain oligosaccharides (sugars) exist in human milk, but not in cow milk. These sugars bind to lectin receptors, thereby blocking the binding of several infectious agents. One example of these sugars’ health benefits is that long-time breast-feeding (over 6 months) has been shown to prevent several types of infections in babies. And in early-weaned babies, if their baby formulas are supplemented with such human milk sugars, their risk of acute childhood leukemia, Hodgkin’s disease, and other diseases will be reduced to the same level as that of breast-fed babies. However, more research needs to be performed on such human milk sugars’ protective effects to adults.
In the human body, there are already inherited genetic modifications as risk factors. The major risk for breast cancer may originate from a systemic infection by BMMFs in the patients’ toddler years through milk consumption. This will result in latency in target tissues. And subsequent infections by the same agent(s) will be neutralized by antibodies. So after an incubation period of several decades, the synergistic interactions between persisting BMMF agent(s) and acquired or inherited genetic modifications will cause breast cancer.
One consequence of the above breast cancer development is that BMMF-containing dairy products will not be identified as risks by studies conducted when the subjects are much older.
This suggested role of BMMF infectious agents can have important implications for breast cancer prevention. Specifically, if BMMFs can be detected during the decades-long incubation period, in which symptoms of breast cancer haven’t appeared, individuals who are particularly at risk can be identified, and preventative and early therapeutic measures can be taken to reduce the risk of breast cancer in their later life.
Estrogens in Milk Promote Tumor Growth and Cancers
A team of researchers from National Cancer Institute, led by Timothy Veenstra, purchased milk from grocery stores and tested its estrogen contents, including estrone and estradioli. As it turned out, the team found 15 estrogens in milk.
Under normal circumstances, hormones are secreted by the body to regulate various physiological functions. However, if the body contains exogenous hormones (hormones which are not produced by the body), they may interfere with the body’s functions.
Estrogens can promote tumor growth in many types of cancer. And even at a low estrogen concentration, this effect can still take place.
Upon conducting further research, the team discovered that estrogen combinations vary widely between different types of milk. For instance, whole milk contains the smallest amount of estrogens, and their amounts are larger in 2 percent milk, skim milk, and buttermilk.
Implications of Current BMMF Research Findings
As aforementioned, early detection of BMMFs could identify individuals that are particularly at risk for certain types of cancer, such as colorectal cancer, so they can seek preventive measures and minimize their risk of developing these cancers.
Currently, the German Cancer Research Center is testing whether interventions for reduction of BMMFs and chronic inflammation will work. If the results are positive, this knowledge will allow the medical community to use BMMF-based therapies to prevent or cure cancers in the future, including colon, breast, lung, prostate, stomach, and ovarian cancers.
According to Professor zur Hausen, the largest challenge at present is to put more emphasis on preventative measures to eliminate cancer occurrence, with any means possible (including surgical interventions). And there is also the need to devise a methodology to achieve long-term protection of patients.
Preventing Cancer
Present recommendations for the prevention of BMMF-related cancers include avoiding consumption of red meat (especially from Eurasian dairy cattle) and milk, avoiding obesity, and using non-steroidal anti-inflammatory drugs (e.g. aspirin). Other prevention measures include the detection and removal of precursor lesions.
A study published in Oncology Reports found that non-steroidal anti-inflammatory drugs, including aspirin, ibuprofen, and other Cox-2 inhibitors, have a protective effect against a number of cancers, as they can reduce chronic inflammation. Specifically, daily intake of such drugs can reduce the risk for colon cancer by 63 percent, breast cancer by 39 percent, prostate cancer by 39 percent, and lung cancer by 36 percent.
According to Professor Walter Ricciardi, at Università Cattolica del Sacro Cuore, Italy, future personalized medicine and good lifestyle choices will help prevent and treat cancer cases.
Do not smoke or use any tobacco
Maintain a healthy body weight
Be physically active and avoid sitting for too long
Have a healthy diet by eating plenty of whole grains, fruits and vegetables, and avoid processed meat and high-calorie foods